
We are rightly alarmed. Indeed, red seems the only color to use to map the shrinking territory where women who are pregnant have an option of access to abortion. As abortion has been demonized as if it, too, were poised to join mass-culture society, and Supreme Court justices resurrect the specter of a society collectively endorsing “abortion on demand” as an apocalypse more apocalyptic than climate change or environmental degradation, the fate of life seems to have been projected to the unborn, even as maternal mortality rates remain staggeringly high across the nation–and seem especially high in those places where the strongest opposition to abortion seems to have arisen on a local level, as a new rebellion in which a substantial, and unable to be ignored, part of America is persistently dedicated to worrying about the fate of the unborn, aggrieved this demographic had been failed to be considered in earlier judicial reasoning about abortion rights.


We have, at the same time, changed how we map access to abortion, now part of our civil society, and also a part that would be wrenching to have invalidated as a individual right. Or is abortion poised to become a civil rights issue, more than a medical one, as it is understood through what this post understands is, rather terrifyingly, a theological context, as it is uprooted and removed from a scientific or medical one?
The color spectrum of these charts flip, but the human impact of how we remap abortion access–or have come to remap it in the United States–indeed seems to bears attention, as it can help us map the situation on the ground. If the header to this post suggests the radical contraction of abortion access in the manner of a geographic warper, similar to the distorted global maps of the prolifically virtuosic Ben Hennig, whose Views of the World are worth perusing to orient oneself to a changing world–but far more dramatically shifting the landscape of access to abortion, in ways that would make maps as important for finding legal access to abortion–suddenly made as complicated a question as migrant routes for asylum.
Indeed, even as the landscape of access to abortion had been creepily and rather creepingly changing by 2014, as a spate of local Targeted Restrictions on Abortion Providers–TRAP Laws–were enacted across much of what came to be called the “heartland” of the nation, the sense of “abortion havens” was mapped already by Business Insider, reflecting how imposition of commercial restrictions on abortion providers had forced many to close–as the introduction on a county and state level of specifics from the width of their corridors, the size and equipment of procedure rooms, and admission privileges at local hospitals, if rarely necessary, imposed costs that compelled many clinics to silently close, even as the “rights” to abortion access were nominally intact–and as no clear “burden” was detected in the partisan decisions and policy moves of state legislatures. The divide between “red” and “blue” states is rarely reduced to abortion, but the notions of family planning, women’s control over their bodies, and the privacy of a woman’s relation to her doctor–if all cast in terms of “cultural” differences among regions of this great nation–are now turned to be resolved, the deck having been fully stacked, to the august institution of the U.S. Supreme Court, having been entrusted with multiple landmark cases in the past to move us to a more perfect union.

Yet it doesn’t seem as if that union’s perfection is on the horizon. The rifts portrayed by Business Insider India in terms of havens in the midst of the hopes to expand health care grew in the United States, but debates about that expansion raged on right-wing television, and among evangelists, was shifting toward the terrifying tones of alarming reds in which we seem compelled to map abortion access as a good that is not only scarce but shrinking at an amazingly unfamiliar and unforseeable rate, as our oceans warm, and fill with more bacteria, and rise, as the polar ice caps melt. It is alarming, because the courts do not seem able to resolve this issue, as the opinions issued on a local level seem incapable of being resolved–and belong do differently framed logics and differently dated discursive fields. One cannot have a rupture, perhaps, but there seem parallel realities that the country is yet again either in danger of entering or existing, which any federal legal resolution by Supreme Court justices seems improbable to provide.
In recent years, judicial opinions have gained a unique status in the headlines of national news. As the courts have gained new status as a battleground where judicial positions rehearse divides in our body politic, the new status of abortion rights as a strategically posed issue has distanced debate from public health–or access to better health care–but a return to “first precepts,” to guiding freedoms, to understand the role of the court on maternal health care practices relate to abortion. Mapping the rapidly shifting nature of this medical landscape as a concerted partisan strategy is only part of the point. For the redefinition of maternal health is nothing less than a deep effort of misinformation, recasting the termination of pregnancy as early as six weeks as a criminal act in the community’s–and state’s–interest to protect, even if the actual “topography” of where abortions occurs has become increasingly uneven.
The prospect of the outright banning of abortion in twenty-six states in the nation demands you to read the current statistics of aborted pregnancies not only as a new “culture” of abortion in the northeast, California, and Florida, but a register of the need that these states meet and provide: if there are “sharp edges” to where abortion is accessed, they reflect population density, poverty, and increased stresses on family planing and growth.

For that map, a poor proxy that shows the steep divides across the nation, many sharply drawn in states–perhaps most unevenly in Texas, with its complex palette of light greens, dark green, and pockets of red giving it a sense hardly of a backwater, but state where, even more than North Carolina, Mississippi, and Georgia, sharp dissonances in the availability of medical care for maternity give it a complexion that seems almost as divided as the nation, and unlike the several states–Alaska and Louisiana among them, but also Colorado and the Dakotas, as well as Florida, New York, and California, of far, far greater homogeneity. Compare this county-by-county map to the prospect of “trigger laws” banning abortion in twenty-six states of the nation, local legislatures have staged a bit of a trap for the vast majority of women nationwide, whose legal access to abortion should the constitutional protections of a right for women to access abortion facilities in their pregnancy fail to sustain a local challenge.
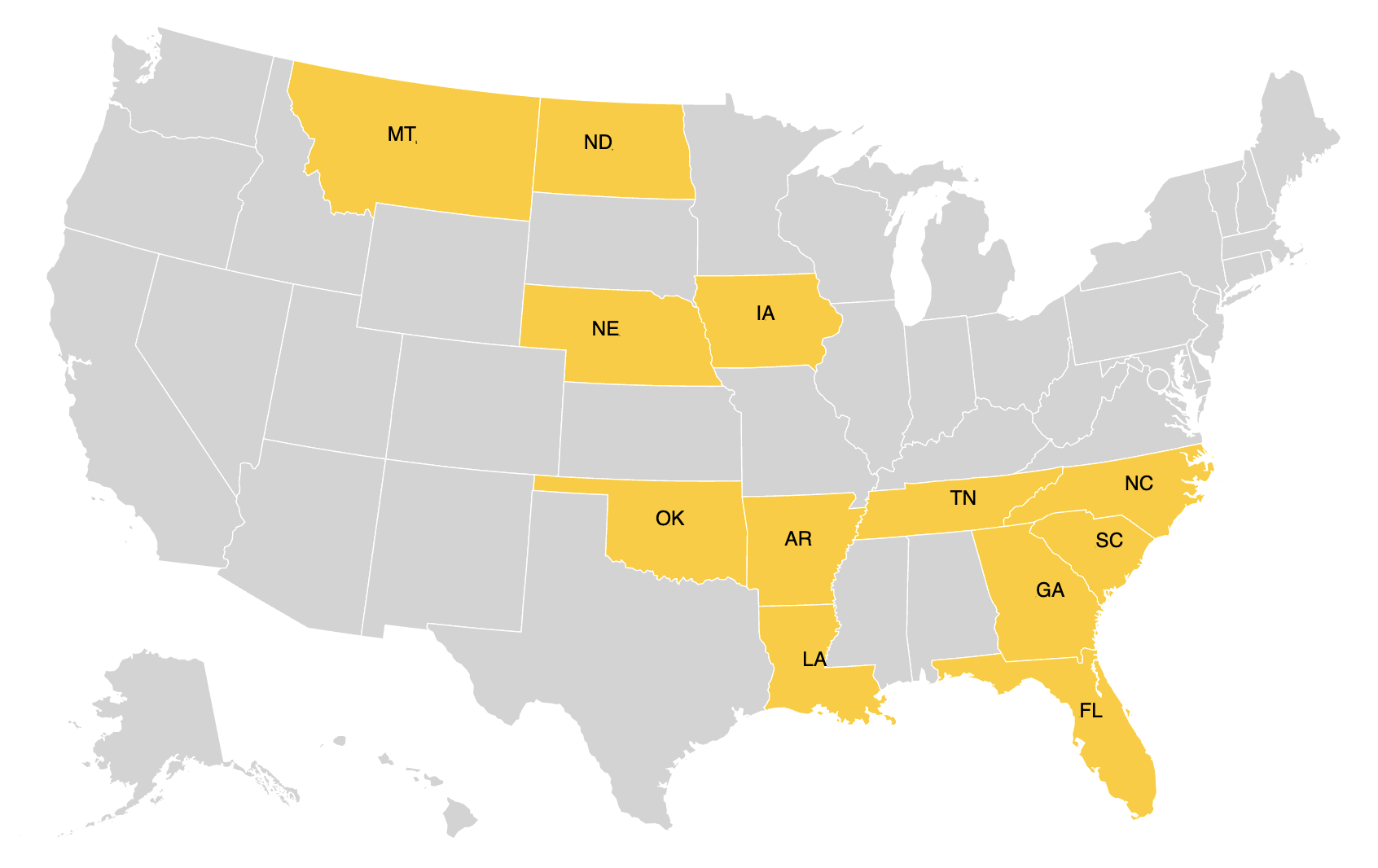
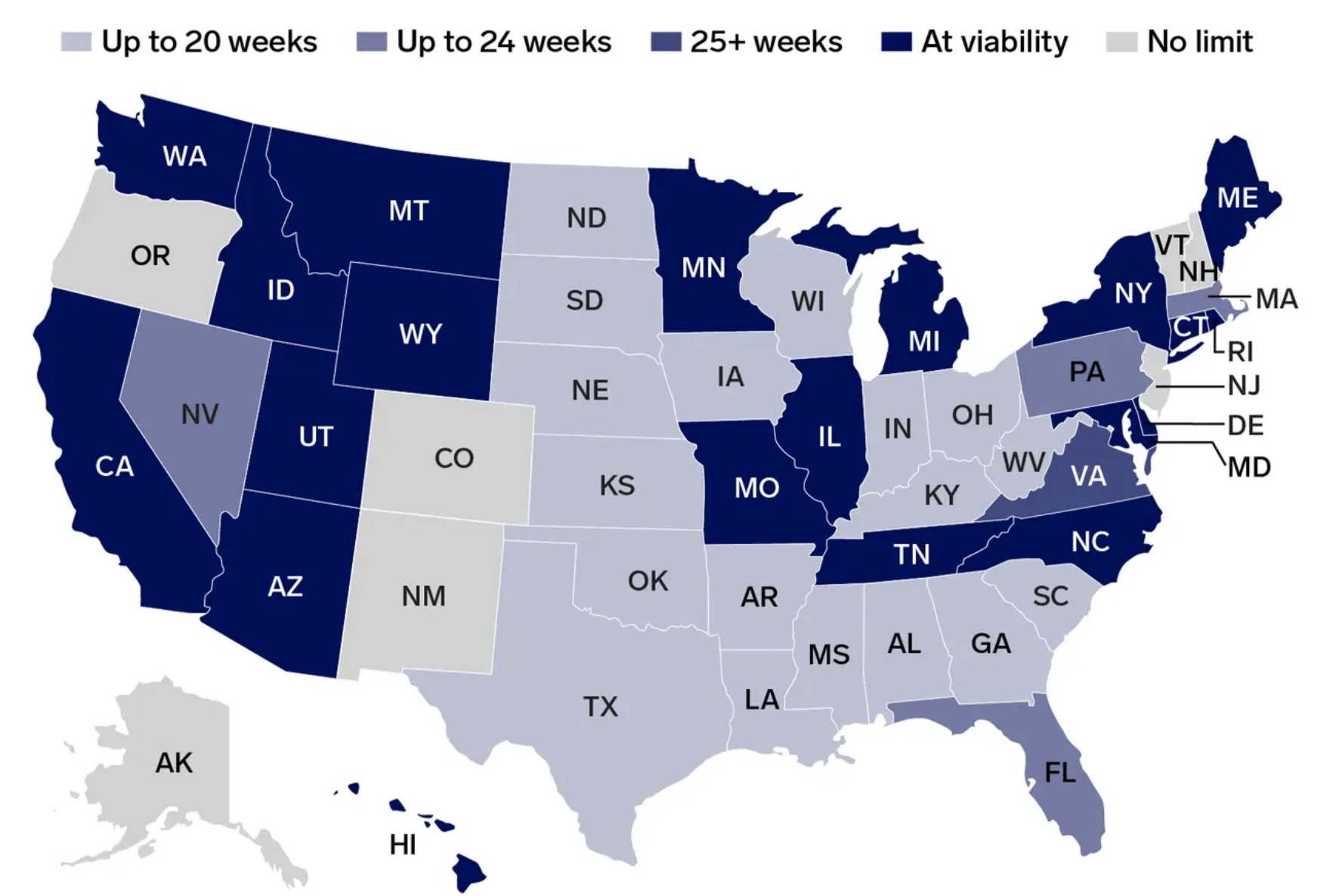
The result is nothing less than a crisis in national health care policies, marking red those states either certain or likely to ban abortion, and those likely–Florida, Indiana, Montana, Nebraska and Wyoming–arrayed in an unmistakable echo of the familiar breakdown of our electoral maps, reminding us of the partisan origins of such a challenge–a challenge that has been reframed not in terms of the rights of women, but the rights of the unborn, as if this new demographic and constituency had been discovered by legal sleuths in recent years.

Guttmacher Institute
Unlike the county-level map of aborted pregnancies, this future map is a prognostication. It dramatically and monitory but maps a landscape of sharp and stark divides, suggesting the remove of women across a sea of continuous states who stand to be placed at a geographic removed from abortion providers without moving themselves. The legislative strategy of rolling back rights that have been presumed for two generations is akin to storming the U.S. Capitol, but reflects a long lain groundwork to secure the state’s compelling interest in protecting the lives of the unborn.
An even starker version of the map by the Guttmacher Institute of amplified monitory value is an image of a brave, new world, with far greater respect for such creatures in it unborn. This landscape, enforced by local legal challenges more arcane assert a compelling interst that the state has in protecting of the unborn, is far more prescriptive than any seen in the twentieth century. It is something of the ground-plan of a strategy that seeks to nail the nation, and its body of laws, to a cross: the red expanse is a sagging net for maternal health care , tracing an opening salvo in a battleground for states’ rights or, more accurately, for the conscription of the unborn fetus in what is cast as a heightened “culture” wars about health care–

–in which the mute protagonist of the unborn fetus is persuasively made a compelling interest of the state. to use its laws to protect, the health or well-being of mothers put aside from any compelling interest that the state might be able to entertain. Unlike the county-level map of clinical practice, which shows variations, the impositions of cookie-cutter prescriptive laws is an intentional an alteration of the terrain, lacking justification or reasoning behind a shift so dramatic, or sense of its implications on the ground in peoples’ lives, out of a deep belief that the previous decision is a pestilence across the land that needs to be contained. But it is also a strategy of promoting the lives of unborn, or of using that line to foster deep social divides.
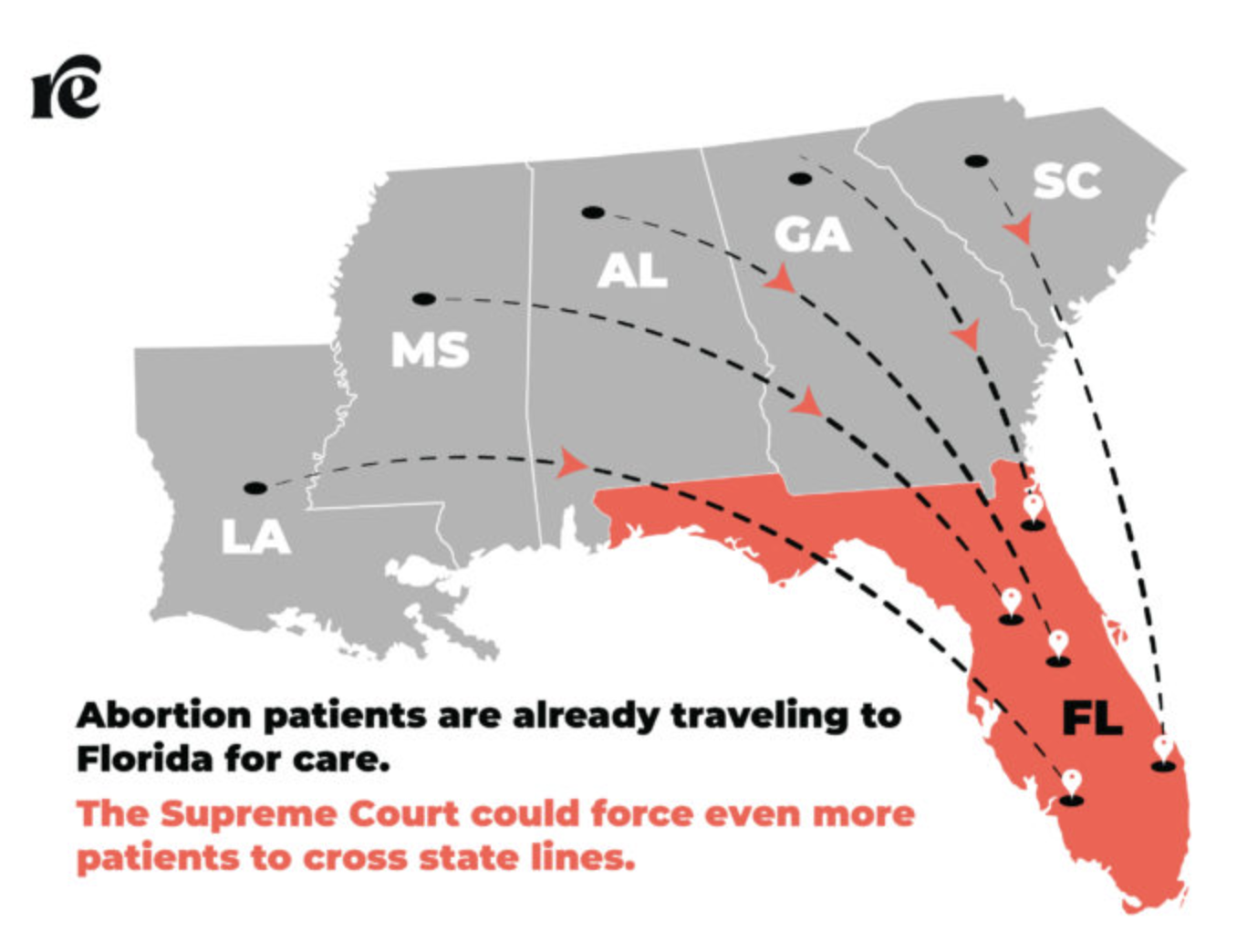
The seemingly scientific justification of reducing the threshold to permit abortion not only removes the practice from the context of maternal health, but suggests “rights” of the unborn that are removed from the subjectivity of the mother, as soon as they are seen–and “mapped”– within the womb. By overturning the notion that the state had a compelling interest in reproductive health, constitutional liberties, or bodily health, attempts to preserve fetal personhood that lacks medical logic has been increasingly dressed in pseudo-scientific garb, by exporting the visual logic of ultrasound to grow a shifting “legal” landscape entertains the rights of the unborn–rather than the burden on women, the health care system, or the law. And if pregnant women were once forced, in the past landscape of the pre-Roe world, to travel outside the nation for abortions–heading to Mexico or Sweden from the east coast and to Japan or Mexico from the west, many states are bracing for an efflux or overflow of women seeking abortion arriving from Texas, Alabama, and Mississippi–including Florida, already emerging as the go-to sanctuary for female reproductive care, given difficulties of border-crossing, with California, Illinois and to some extent New Mexico more costly alternatives.
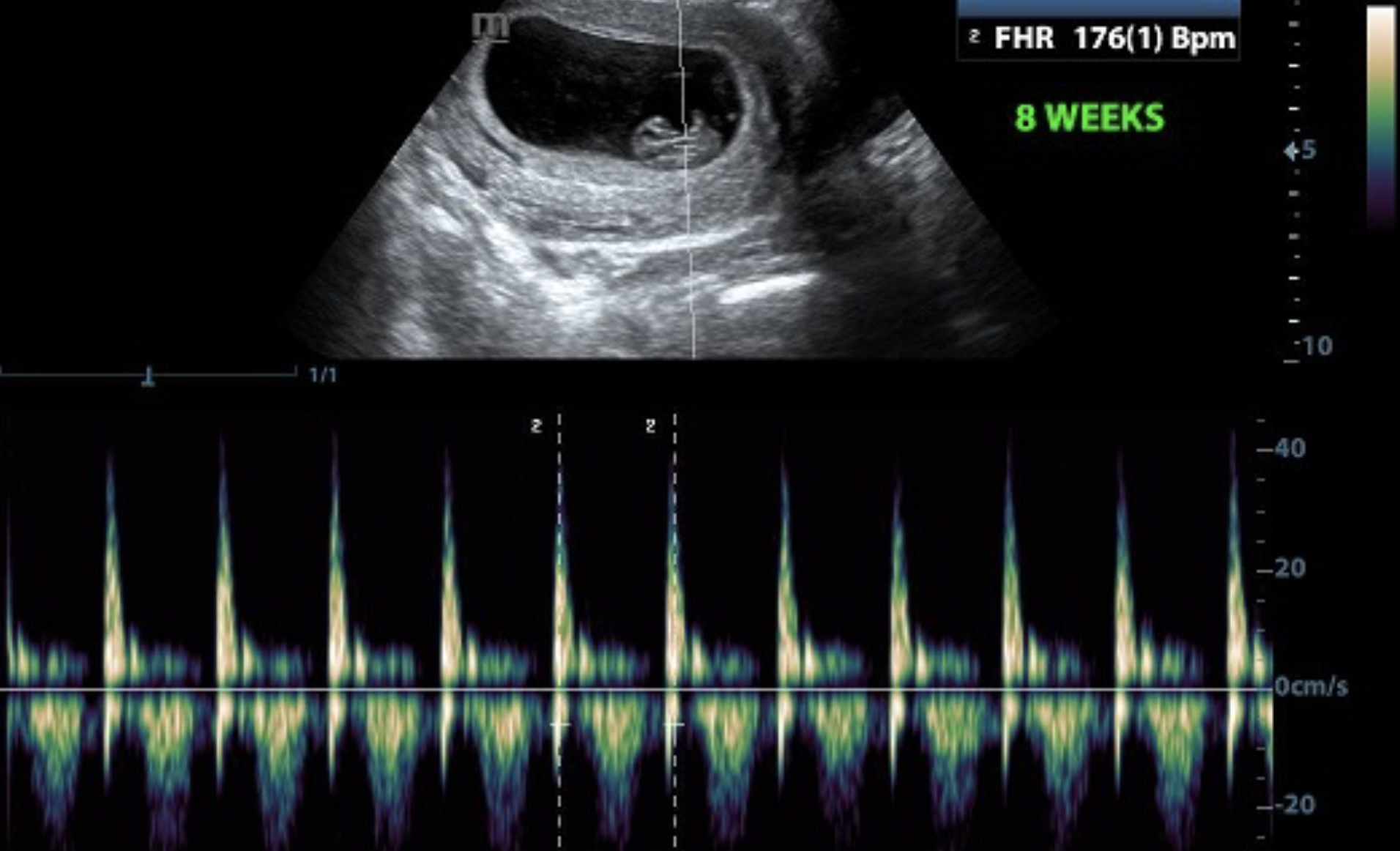
The current attempts of states to devise local workarounds that evade the constitutional right of access to abortion–and guarantee of access as a binding precedent of the court–has come up against loggerheads with the concept of the freedom of “unborn children” posing pressing questions of what is a “compelling interest” of the state in a fetus before life can be sustained outside of the womb. The recent focus of on the heartbeat, or rather the appearance or perception of the heartbeat, as an index or sign of value–if without basis in medical science–has become a new basis to increase the burdens on women in most states to access maternal health. For the designation of cardiac contractions as evidence of a “person” or a soul that in the interest to the state to protected is, in fact, a terrifying smokescreen for the radical contraction of a pregnant women’s rights.
In ways that have framed the question of access to abortion in the nation in terms of how they are addressed in the U.S. Constitution–reticent or silent of any issue of women’s health–the question of what the role of courts is in preserving states’ rights to restrict access to abortion and health care, or to defend the access of women to be able to terminate a pregnancy, has placed undue stress on the place of legal reasoning in determining access to maternal health care. The current drive to regulate abortion, itself a pronounced response to the expansion of the health care markets from 2008, have become a national divide of striking proportions, so much that they are cast–wrongly, for this blogger–as a cultural divide.
But the storied cultural divide of abortion is a deeply geographic one, as we have long been habituated to preserve access to abortion since reproductive rights first came under attack before Casey, in the 1990s, as preserved by cities as the National Institute for Reproductive Health shifted their ground game to ensuring that cities–not necessarily where abortions were most in demand, but where voters and elected officials were far more sympathetic–lived. As if the riots of January 6, 2021 attempting to stop the end of Trump’s Presidency by a show of force in Washington DC, the latte-drinking liberal city-dwellers before their laptops–a tired political cliché we all love–is also apt. For it is among urban audiences of a certain age that a political precipice seems to have suddenly reached, as constitutional grounds for health care shifted beneath their feet.

The protection of “abortion rights” by local safeguards in cities emerged in dialogue with, to be sure, the expansion of local restrictions on access to abortion from 2010-2016, and the cumulative weight of three hundred and thirty measures to restrict abortion, and a logic of shoring up rights in a deeply divided polity where rights of migrants, unhoused, and poor were feared to be evanescent or at risk, and the law no longer a stable fabric. Urban preserves where women’s rights to access maternal health care were predominantly coastal, and often, far removed oases from the sites lacking sanctuaries of legal protection, revealing the shifting palette of access to “freedoms” protected in the constitution by standing legal opinion. From 2016, at the end of the Obama era, as battle-lines over Obamacare concealed fights about abortion, reproductive freedom was a mixed bag across the country, reflecting in terrifying ways the 2016 electoral map of a broad continuity of red states as a mythical “heartland.”

The new ground-game of shifting the threshold of permitting abortion–imagined as enacted by local legislatures–suggests an endgame of a territorial fragmentation of once-universal rights to access abortion would shift the clock back five decades overnight. The ground-game is swift, and demands to be drilled into, both in Texas, and in other states, as it may well be poised to be recognized as law of the land, setting off tremors of health care and desperate searches for access to clinics–or potentially unsafe, if used as a last resort, abortion pills designed to simulate miscarriages–across the land, placing pregnant women at only greater risk.
The swift pace of shuttering abortion clinics in Texas by local legislation–magenta dots marking the actual closures of clinics offering abortion in Texas due to local laws, chipping away at or decreasing the actual liberty of access that is ostensibly the law of the land some years ago.


The map can be drilled down into far more deeply to describe the distance at which local laws have “placed” women of child-bearing age from clinics–creating a skewed topography in which, by 2014 data, women were compelled to travel nearly two hundred miles, at their own expense, to obtain abortion services, curtailing health services that were available to women and the abortion “deserts” that were quickly–and intentionally–created across the state.
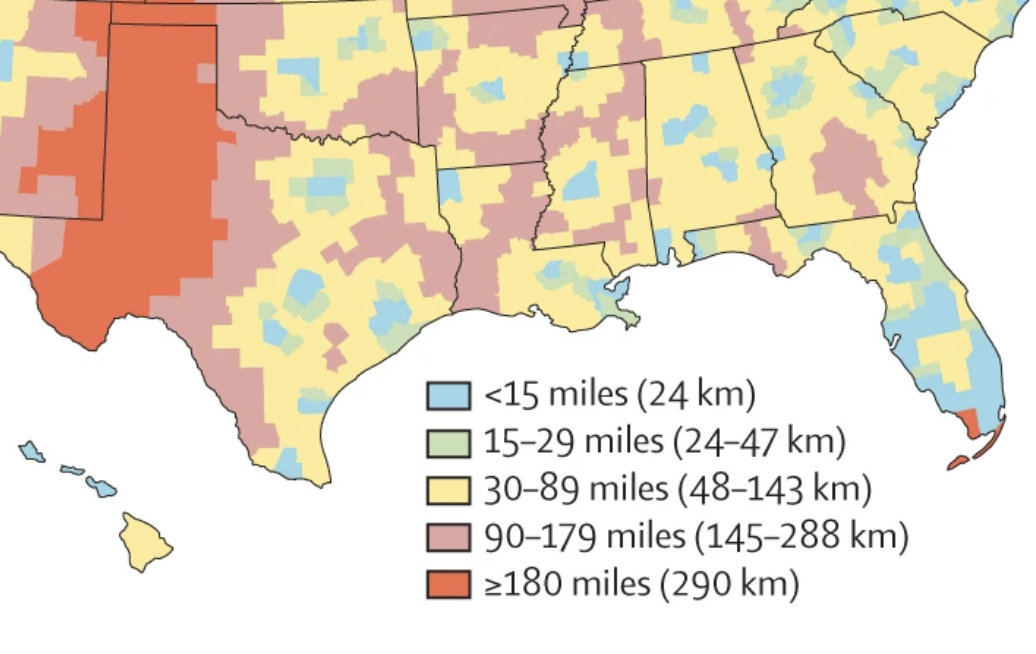
The burden of such restricted access to clinics that can offer abortion in a substantial area of the state where women would be demanded to travel upward of 100 miles to a clinic has created exactly such a burden, but has emerged as a state’s right, by expanding the “compelling interest” of state counties to ban abortion not by the yardstick of the trimester of pregnancy–a standard in Roe v. Wade or fetal viability, measured by twenty-three to twenty-four weeks after conception, permitting the procedure up to that non-arbitrary date. Yet the unequal remove of women from abortion providers seems a burden as undue as an other, especially on women without the economic option for extensive travel to locate a provider within the state’s bounds–or, as seems poised to become the need, outside of them.
Should Roe v. Wade fall, and the constitutional right of women enjoy to access abortion as a form of maternal health care vanish overnight, “tigger laws’ already on the books would prompt an immediate jump of average distances of women to abortion clinics from 36 to 280 miles, as 41% of women in the United States would find the nearest abortion clinic closing overnight, no preparatory window or period of adjustment–or alternative–in place. The ground-game, rooted in the election of local Republican officials of a pro-life strip on city councils and state legislative chambers, is an open attempt to erode the affirmation of rights that cut against the , creating something akin to “cities of God” that follow outdated norms of the protection of unborn lives by using the odd index of the sonograph as a proxy for what medieval theologians called “ensoulment,” adopting Aristotelian science to gloss scriptures, in a proscriptive model that has little relation to medical science or health care, or the freedoms to privacy and self-determination that were once protected by the Constitution.
It was another helpful service to American webizens, the Decolonial Atlas, your place to go for go to remedies on the web, posted a travel map of routes to abortion providers in southern states, collating affordable transit routes to clinics that would provide abortion services–services that were still technically “legal” but out of the range of many, and prohibitively expensive for most in need of them. The bus routes women might take to reproductive health service centers in many states–Illinois; Missouri; North Carolina; West Virginia; Tennessee; Florida; South Carolina–would be open, but prompted questions of economics and opportunity. The further question of the fear of undocumented being stopped by a zealous Border Patrol, should they move across and be stopped at checkpoints en route, would be wary to avoid. The feature lending prominence to the “border zone”–an inheritance of the over-policed border of the Trump Presidency–was kept from an earlier map that had gone live September 4, 2021, setting a six-week window for abortions as state law overnight, panicking women across the state who had suddenly lost access to a crucial piece of their health care.

Already, the mobility of women seeking abortion had seemed a steep threat to many in Texas, where an undocumented woman seeking an abortion might risk deportation for traveling from Laredo or Corpus Christi to Health Care Centers in New Orleans or Jackson, or even on her return from Austin.

nTo be sure, the heightened mobility of women seeking abortion is a new iteration of the regular plans that, before Roe, the Society for Humane Abortion offered those with sufficient means to travel to doctors outside of the United States’ borders–from the west coast, Japan was a destination of choice from the late 1940s, if not Mexico, helping some 12,000 with their passage to clinics outside American territoriality. These burdens of travel, indeed, were no small part of the logic for revisiting the placement of “substantial obstacle[s] in the path of a woman seeking an abortion of a non-viable fetus,” a tricky problem that seemed a necessary point of consensus in the modern world of birth defects, often due to other medications. Yet the image of increased out-of-state travel and the burden that this would place in the paths of women was not clearly addressed by the Court, nor does it seem to have since. The rather terrifying image of freedom to access abortion being curtailed or removed due to the orthodoxy of a majority of justices recalls the pamphlet of the same organization protesting the right to “breath unpregnant,” wom the Society for Humane Abortion would happily send forth to another shore, her rights and liberties curtailed in the United States.

While Roe resulted in the reasoning that voided “the purpose or effect of creating a substantial obstacle in the path of a woman seeking an abortion of a non-viable fetus” as placing “undue burden” reflected a standard that a burdensome restriction of constitutional rights could not be imposed by states, a finding of the late nineteenth century. The unconstitutionality of imposing an burden by any state in the union from the late nineteenth century: the standard applied in 1992 preserved women’s right to terminate pregnancy before viability does not relate to counties, only recognizing rights to ban abortion after the “viability” of a fetus outside the womb, save when the pregnancy endangered the mother’s health, and not using the rhetoric of personhood to describe the unborn. Definition of a burden as “undue” “either because [it] is too severe or because it lacks a legitimate, rational justification,” posits protection of rights of mothers, but are argued to deny the rights of “unborn.” But the shifting global limits on abortion are practically unique in multiple standards that are on the books in the United States, with some states holding no gestational limits, and some shifting them to a window as small as a month and a half, producing a forced mobility for obtaining abortions in the horizon. Perhaps this is all to familiar in a nation that experiences multiple realities and opportunities–and now liberties– for different levels of wealth.

Put another way, equal access to abortion is no longer the law of the land. And the drilling into the data of the multiple laws that have been locally proposed in states reveals not only a partisan strategy, but a deeply unworkable system of different tiers of maternal care. Since 2011, these rights have been attempted to be defined nowhere more prohibitively than in Texas. In the nation, over half of the closure of clinics that offer abortion services to women have closed by local legislation, in a concerted partisan push unfairly argued to reflect “local cultures.” The partisan nature of closures has been a template for “red state” policies from Iowa to Ohio to Louisiana, changing the on-the-ground landscape of access to abortion by forcing many closures due to safety violations, difficult work environments, and business decisions,–already a bleak landscape for maternity care for over the past decade, in eery contemporaneity to a public health option that would provide more maternal health options.

The opposition to abortion that focuses on the “unborn”–and the humanization of the heartbeat of the unborn, rather than the fetus–has become one of the more striking defenses of pseudo-freedoms. These are freedoms not ever articulated in Enlightenment thought, and foreign to it, from freedoms of belief, to freedoms of owning automatic rifles and military-style arms in one’s home, that extend to the protection of freedoms of the unborn. Such freedoms are resonant with full-throated opposition to mandates for mask-wearing, hand-washing, social distancing, or vaccines. The spread of challenges to the access to abortion and abortion pills across the nation deny the life-changing role of pregnancy on all women, and the greater dangers that childbirth–hardly a risk-free event!–imposes on women, let alone the dark topography of sharply disproportionate and increasing rates of maternal mortality in many of the states that have restricted access to abortion.


The freedom to restrict abortion is similarly anti-scientific, and theocratic, strategically removed from the undue onus that state laws against abortion would have on women–especially if a good share of the clinics providing abortion to clients–sites marked below in orange and black–cease providing clinical care to women. Although it is argued that this will shift demand to mail-order abortifacients, safely used only in the first ten weeks of a woman’s pregnancy but providing subject to local and state provider restrictions, 99.6% successful if used at nine weeks from conception or less, and require in-person–consultation with a physician to be prescribed in fourteen states that have enacted restrictive abortion laws–including Texas, Oklahoma, Mississippi, Alabama, North Carolina, South Carolina–of thirty-three states permitting only physicians to provide mifepristone, creating divides to access “self-managed” that are poised to sharply grow along clear fault-lines, and perhaps creating a undue underground economy for abortifacients of unseen proportion; states limit abortion pills to being dispensed by physicians, despite that they are as effectively dispensed by nurse practitioners or midwives, create compromised access to health care in thirty-three states.

–and five states that have ban telemedicine for medication abortions, including Louisiana and Arkansas.
The result is a terrifyingly unequal deep, dark landscape distant from abortion facilities, whose loss is indicated by dense orange colored dots, suggests the severe restriction of health options for pregnant women that would result from overturning Roe v. Wade. Twenty-two states have adopted laws that the overturning would ban abortion within their borders.


The undue burden on women who unable to provide the option to terminate their pregnancy before viability would grow in such ‘abortion deserts’ and impose a significant burden on states that affirm abortion on their edges, whose surviving centers would face ethical problems of facing a greater demand–if women travel to them, the states are potentially now exposed to the legal suits for violating laws restricting women’s access to terminate a pregnancy they do not want. Concerns that overturning Roe would increase travel to California to seek an abortion by almost 3000% is born out by the map below–restrictive laws in other state long increased out-of-state clients in California; increased demand for access to abortion from women residing in state laws restricting access to abortion would expose California to legal action for violating their laws.
The urgency to address the demographic of the “unborn” recuperates a category from the thirteenth century that enjoying a recent resurgence with the legal parsing of personhood. But while one spoke of the “fetus” in the 1970s, when Roe v. Wade was decided by the Supreme Court, the shift to “fetal personhood” expressed by 2018 in Iowa, then the state with the most restrictive abortion laws yet, which made abortion illegal after a fetal heartbeat is detected, skipped over the question of a woman’s right to abortion, but expanded the ability of states to “regulate access to abortion” to the extreme, by permitting a ban on abortion earlier than most women would be likely to know they are pregnant, putting Iowa in the range of states with court-imposed restriction to abortion, contraception and reproductive services. While not framed as about sexual freedom, anxiety about women’s sexual freedom in 2017 and moral arguments led many central, southern, and midwestern states to adopt court-ordered restrictions parallel to the expansion of health care that included access to abortion–
-and must be seen as a resistance to it that set the basis for the “red states” which emerged as a united front in 2016 and the pro-life candidacy of Donald Trump.
The majority of states in the union adopted restrictions without any basis in scientific evidence at all, or clear roots in jurisprudence. The restrictive laws that were predominantly of proscriptive cast, betraying a terrifyingly theocratic origin in identifying the origins of “life” as a focus of judicial inquiry in a neo-medieval cast. Is establishment of any “heartbeat” law not in itself an undue burden on women, inviting the undue burden of placing a ban on abortion before fetal viability, that would demand to be struck down as such? While placing burdens on women throughout a large number of states, the local laws create new concepts of strict scrutiny around heartbeats, arbitrary weeks since conception, or the detection of reflexive movements in ultrasounds, all of which are coercive controls that serve to undo the undue burden concept.
1. Abortion was historically challenged by the medical profession as a way to restrict the role of women healers–and female agency–in the nineteenth century. But the search for legal obstacles to abortion is wrongly treated as a return to first principles but a shift in freedoms of access to health care. But the question of fetal “personhood”–or indeed of personhood of the unborn–dispensed with the very logic of potentiality that Roe left in the law by reserving for the state an “important and legitimate interest in protecting the potentiality of human life from the twenty-fourth week of pregnancy,” dissolving that interest in favor of shifting the question from “potentiality” or a “Golden Rule” that grew out of attention on the fetus as a focus of protection; the expansion, due to stem cells, in vitro fertilization, and fetal tissue transplants on the moral status of the embryo as a subject in place of the woman’s right to access abortion or abortion providers.
While Aristotle was primarily concerned with the emergence of a rational soul, a concern that was adopted by twelfth century theologians who embraced his notion of the formation of the soul in the developing human embryo—the vegetal soul, the animal soul the intellective or human soul–the notion of personhood dispensed with the epigenetic stages of ensoulment, but focussed on vital signs located in the heart as a sign of life, independent from science, but reflecting the technologization of birth. The adoption of policies hostile to abortion rights in 6 states and of laws extremely hostile to abortion rights in 23 states) to abortion rights, and the hostility expanding to Iowa and West Virginia for the first time, created not only a new map of abortion rights, but mapped the origins of personhood in the womb. The result, according to the Guttmacher institute, placed the majority of American women able to bear children in states hostile or extremely hostile to abortion–without rooting their arguments in science.

The defense of the “unborn person” flew in the face of science, beyond questions of cultural difference, from “mandated ultrasounds” to regulations on abortion clinics, including removing clinics from Medicaid, to, in Alabama, a state-wide ballot initiative to agree that personhood began at conception, the Human Life Protection Act, signed into state law in 2019, that “defines all unborn children as humans”–and allowing no exceptions for rape or incest. The bill was adopted only to encourage the Supreme Court to revisit Roe v. Wade around the question, in the word’s of its sponsor of whether “the baby in the womb is a person.”
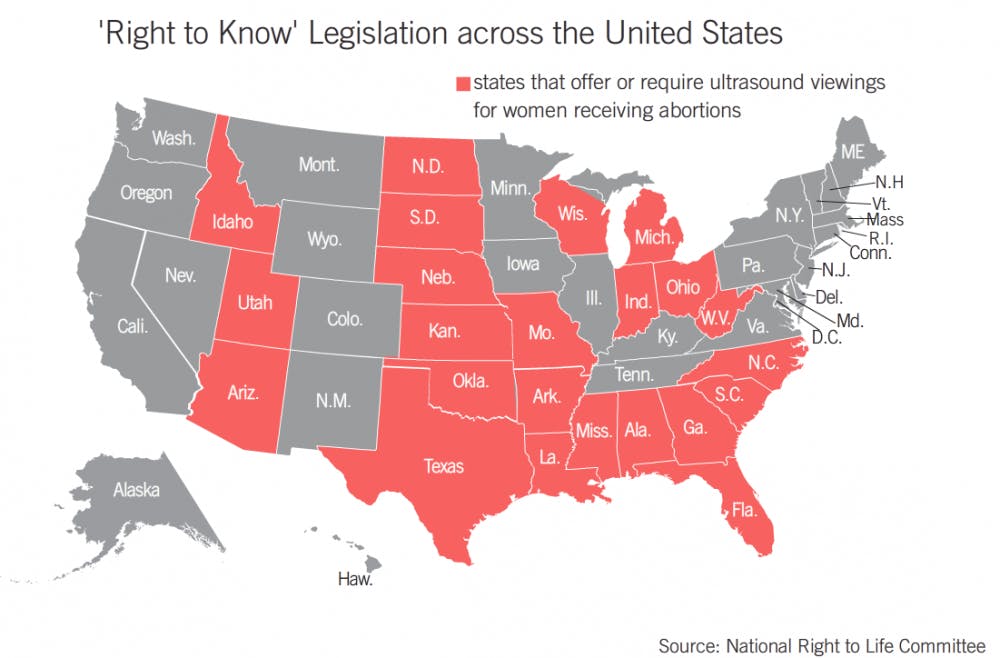
For by redefining the fetus as a “life,” with freedoms and liberties attached and pursuant, Iowa’s legislature abandoned the standard of viability outside of the womb, asserting that the unborn is a person, and abortion tantamount to killing a life, as if “the burdens of carrying a child to term [could] justify the killing of a child,” per the lawyer representing the state of Iowa in 2018. It takes arguments of the potentiality of the unborn to the extreme, not discussing the Thomistic idea of potentiality of human life recently promoted by Catholic theologians as a middle ground, but mapping the heart of the matter–the heartbeat–the visual evidence of personhood. Fueled by the affective relations of ultrasounds that offer the “science” that seems to sever the personhood of the “unborn child” from the standard of viability that had set the threshold for up to what point the protection of a woman’s access to abortion was permitted by constitutional law. The rise of proscribed ultrasounds across multiple states reflect the new focus on personhood and heartbeats, whose mandated display and discussion provided a preventive basis for persuading those seeking abortion to forego the procedure.


Cast as a “Right to Know” legislation that was introduced in Pennsylvania in 2012 mandating all women who are seeking abortions to view the ultrasound designed to determine the gestational age of the unborn fetus–a means of placing the abortion in a window of viability–offered all women seeking an abortion the “right” see the image, and to hear the heartbeat, offering a new way to map life and epigenetic questions of ensoulment around the “beating” of the heart, although no ultrasound was mandated in states protecting abortion rights.
The states that have pushed back on this definition for one more consensus hardly appears scientific, gives a scholastic sense of ensoulment first articulated in the thirteenth century contemporary relevance, mapping the unborn on an ontogenic continuity of personhood that reduced the concept of viability that the court once embraced to a relic as quaintly outdated as Plessy v. Ferguson’s ruling that segregation did not violate the fourteenth amendment. The insistence of a Justice on the highest national court that the compelling interests of the “unborn” has become grounds to review the liberty of women to access abortion prior to the line of fetal viability outside the womb. Defining personhood from conception has pushed back these freedoms to the unborn in ways without legal precedent or, championing the court’s role to represent the interest of the unborn, preventing violence against those being carried to term, handing down a sentence against all women asked to carry a child to term.
The imaging tools of the ultrasound after all transformed the fetus to a “baby’s head” and “baby’s heart” able to be recognized on the screen, and indeed labeled for identification, in ways that seemed to deliver a deeper truth, in an age when we have difficulty distinguishing representation and reality, expanding the case in the courtrooms that the presence of a fetal heartbeat offered incontrovertible evidence in a court of law that a “a human child with a heartbeat is a living child,” even if few judges in Iowa were ready to hear the argument, if the state’s lawyer refused to accept that the fetus with a heartbeat was a “potential life”

Although Roe v. Wade has been discussed as precedent for decades, occasioning only recently clear skepticism about reducing women’s right to abortion by restricting the window of “viability” of the unborn to twenty weeks, in North Carolina, one to two months less than the usual 24-28 weeks, but currently nineteen states take the date as the cut-off for access to abortion, in ways that have made the former standard of viability to seem virtually arbitrary, rather than grounded in embryology. The emptying of any embryological standard–or indeed medical expertise–has come to be cast as a “cultural divide,” out of the court’s sphere of decision making or competence, with seven states on board to limit abortion to the greatest extent possible to twenty weeks: Kansas; Kentucky; Arkansas; Louisiana; Missouri; North Dakota; and Ohio. The critical curtailing of this access in Iowa, the site of the first primary to select the United States President, suggests an undue prominence of an ambivalence to abortion in our national politics.
The effective reframing of rights to access abortion as a question of “states rights,” rather than public health, and of local “liberties,” makes Texas the perfect site at which a national debate about abortion access can be balanced, however, as the current debates on similar local laws in Mississippi–reducing the window to fifteen weeks–it almost even left Chief Justice Roberts flummoxed to ask if the window would always be effectively arbitrary, as if the number of weeks were divorced from a woman’s body or a woman’s womb. The voiding of any constitutional right to abortion in four states of the deep south–Alabama; Louisiana; Tennessee; West Virginia–already pushed the debate away from constitutional rights. Yet the result of shifting the “burden” pregnancy places on women from the nation’s courts suggests a seeming time warp for much of the country, maybe not to the the 1200s, but at least to the years before 1972 at the stroke of a pen–or a verdict of 5-4.
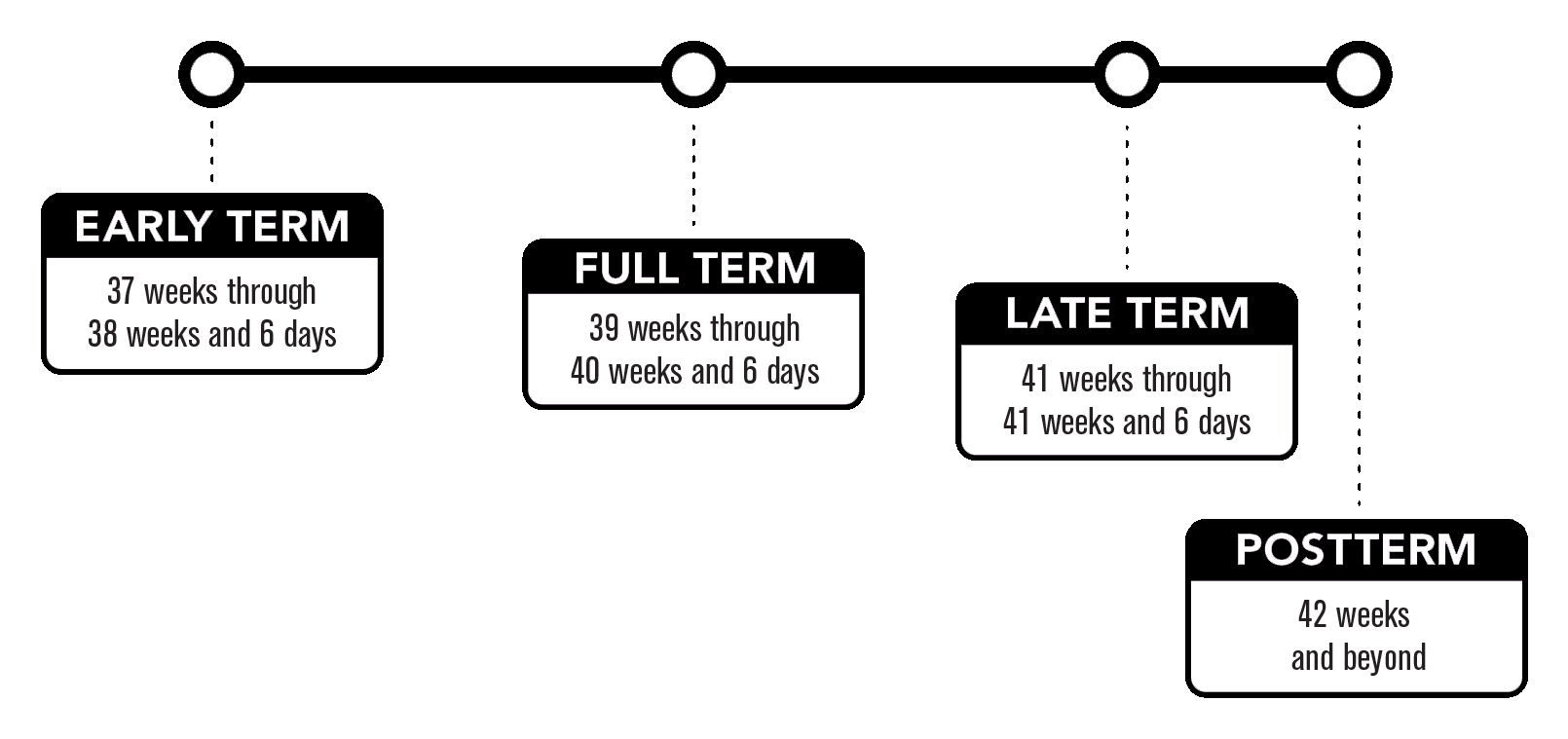
While created “full term” pregnancy created a temporal standard to determine the viability of the babies born at an early date–before thirty-nine weeks since conception–to breath, feed, and regulate their bodily temperatures outside of a neonatal unit, the pronouncement of the “the fetus has an interest in having a life” effectively unties the umbilical cord though which blood flows to the liver of the unborn infant as if it were a Gordian knot, lest harm come to the undefended embryo before it has fully developed.
The inclination of the nation’s highest court to remain “neutral” to the “culture wars” about abortion aims to shift access the legal grounds of women’s access to maternal health care. The issue has become so overly politicized that the court should be compelled to defend access maternal health care, lest the “full term” of pregnancy be imposed as a sentence on all fertile women in the nation.
So little grounds exists in the nation about access to abortion–and such open hostility from the “states rights” region of the deep south, accustomed to defend their local traditions without regard to their hurt. So it was no surprise, in many ways, that freedoms of the unborn emerged as a strategy to circumscribe access to abortion rights, and indeed affirmed a logic to revisit the constitutional rights of access to abortion. Argument so old they might be dated to Thomas of Aquinas who, following Aristotle, saw conception as completed six weeks from conception for boys, and about thirteen for women, may inform the rationale for removing access to abortion after six weeks. But the old arguments of medieval science bottled in legalistic arguments may seem watertight, once cast in terms of “states rights,” the arbiter of access to health remains a national question, and not only in Texas–especially given the deeply disturbing ways that the passionate hostility to abortion eerily echoes an electoral map.


2. How did this come to be so effective? The territorial divide into “red” and “blue” states is almost a shorthand for anger on the ground at the expansion of access to abortion that Roe v. Wade guaranteed for all women when it historically struck down Texas laws that criminalized and prohibited access to abortion in 1971. The fight in Texas was not only with a long memory of the striking down of statutes fifty years ago, but the reversal of a decision that has been instrumentally used to foment a fault-line of red and blue states around foundational principles, rather than health or women’s rights to access comprehensive health care. Only in 2020, the fault lines that would have guaranteed an electoral majority for the Presidency and future nomination of Supreme Court justices did not hold–if it almost did–as new bellwether states like Georgia, Virginia, Arizona and Wisconsin overcame an often dominant hostility for a greater good.
The critical drive for the Trump presidency might be traced to a single moment in 2016. The declaration of a candidate for President who in 2016 promised the nation that, if elected, he would “return Roe v. Wade to the individual states” to decide and that, if he was elected, the reversal of Roe v. Wade would “happen automatically” as he would support the nomination of pro-life justices, once “we put two, or, perhaps, maybe three, justices on, that really is what would happen.” Trump’s vow that the decision will “go back to the states” expressed in nuce the opposition to keeping abortion within a program of national health care, and made with his identification as pro-life, he left Hillary Clinton rather wide-eyed just before Halloween 2016, as she must have contemplated that reality and its popularity.
John Seago, legislative director of Texas Right to Life, who has coordinated on the ground efforts to expand pro-life movements, didn’t even wait for the full court to pronounce. He seemed quite content to entrust Catholic Justice Alito to represent his organization’s interests, deferring to the sole Justice’s judgement with false modesty, as if addressing an intercessory advocate to resolve his organization’s longstanding efforts to use state laws to reframe abortion from a federal or constitutional issue: “We are [just] hopeful that Justice Alito will examine why the [request to stop the law being enacted on constitutional grounds] should ultimately be dismissed,” he noted at his luck at having a like-minded member of the court poised to affirm Texas’ right to ban abortion for all practical purposes as a felony. Texas was not at the vanguard of eroding rights for abortion, but it was perhaps in the front lines of doing so as an offense of the public good. And Seago proclaimed Alito as an intercessor of sorts for affirming the state’s legislators’ ability to restrict access to abortion fit in a general process and broad strategy Antonin Scalia framed in a living legal tradition of dissent to Roe v. Wade that has emerged in recent months.
The new fight to curtail constitutional rights of access to abortion as a form of reproductive health care chipping away at consensus on women’s rights to access abortion as a question of privacy–about which the court should be neutral–to allowing a local activist judiciary to question the thresholds of such access. Since this constitutional right for local adjustment of the national law was effectively sanctioned in the 1992 verdict permitting local states to restrict women’s right to privacy that has already eroded the place of access to abortion within public health framework. The increased activity to disrupting national consensus on health rights became increasingly bitter during the expansion of public health insurance, which reposed the question of funding for abortion on the front burner of national debate, and energized local opposition to abortion among local groups. The convergence of an eager local resistance to include abortion within reproductive health care and restrict abortion in Texas is in the news. But Texas is hardly an outlier atypical in the terrifying restriction of reproductive rights. Rather, it is one of the more legally creative sites of resisting access to abortion, perhaps most ready to articulate resistance to a national law and more ready to agitate for local control of the law of the land by extreme legal experimentation.
As much as Roe v. Wade is settled “law of the land,” the dissonance and pitched battles over access to abortion are less based on values of “human empathy” to the rights of the unborn–a specious argument that seems dangerous terrain to enter–than the deeply compromised terrain of reproductive health that women face across America, where women’s rights to access to abortion has needed to be defended. If Texas was long a lynchpin of sorts in this battle, divided by access to clinics and sharply divided as to the place of abortion in reproductive health care, the divided politics and demographics of Texas may conceal how deeply the curtailment of women’s access to abortion underlies division into “red” and “blue” states, as much as other ideological lines of debate: while this is not prime, the deepest heartland of deep red states map surprisingly clearly onto the diminished reproductive rights in telling ways–
–as those states that protect rights to abortion through “viabilty” established in Roe, or even extend the access of women’s protected rights to abortion beyond that date are more solidly “blue” and dominated by democratic legislatures.
3. How did the state become such a vanguard of the erosion of abortion rights and attack on science? The prominent place of Texas as a vanguard and a lynchpin of the curtailment of access to abortion may be but the first in the sustained curtailment of rights to abortion, questioning what constitutes an “undue burden” on women with increased aggression and alacrity. Does this pressing urgency partly not derive from the deep enjambent of attitudes to abortion that distinguish the state, placing the issue of abortion as a hot button issue that demands attention as it seems to lie, locally, at the enter of the culture wars?
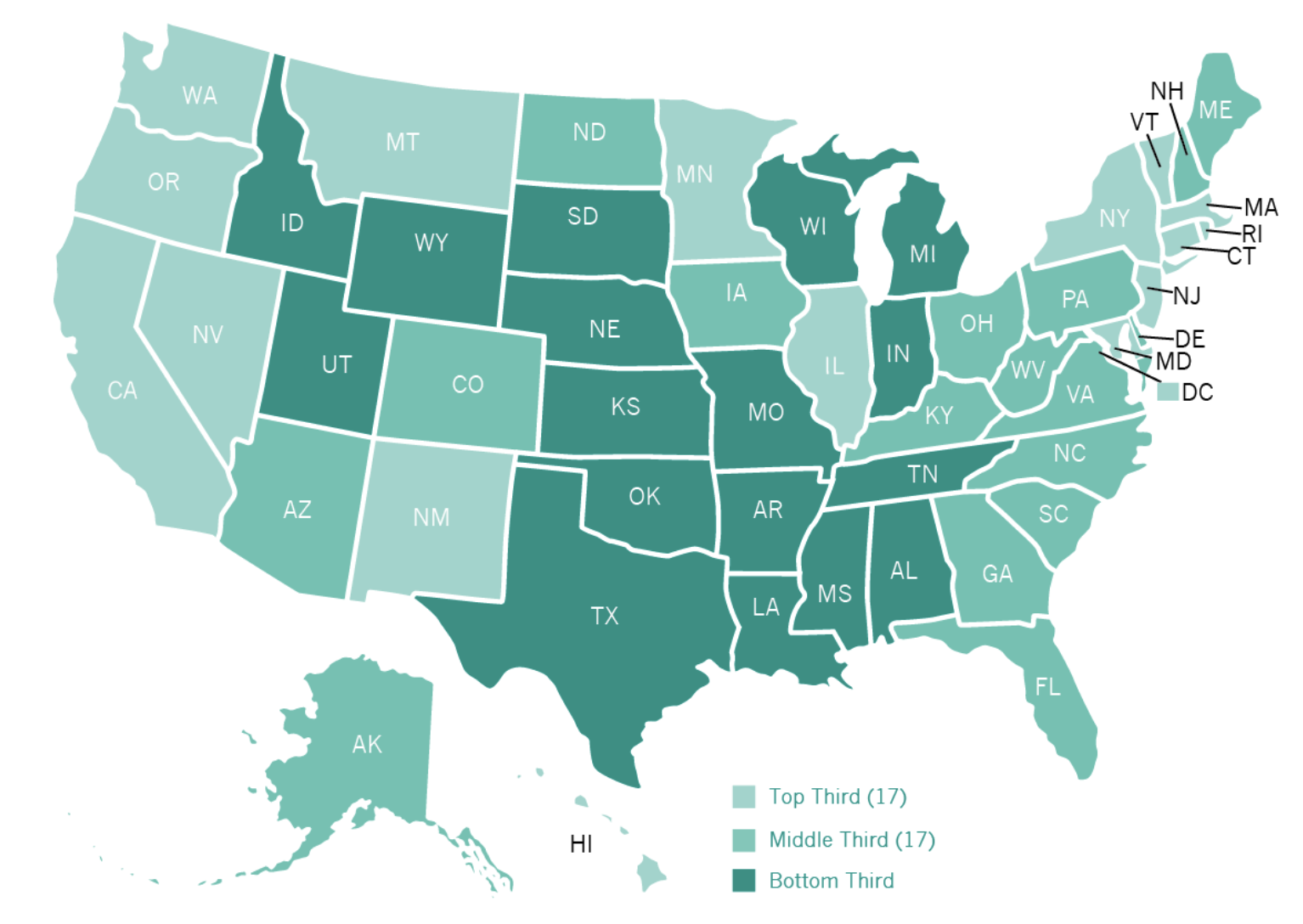
The state has one of the sharpest discontinuities in rates of abortion per pregnancy in the nation–juxtaposing counties with rates cresting half of all pregnancies with the majority of counties showing rates about 10% or even half–in ways that may make the state one of the sharpest sites of dissonant practices where cultures felt invaded by a new culture of maternal health care in Houston, Dallas, San Antonio and El Paso, pockets of higher rates foreign to the surrounding state–unlike, say, Florida, Washington, or Massachusetts, but akin to some parts of western New York, Oregon or Maine.

Johnston’s Archive, 2011 (published 2019)

This was combustable grounds for finding support to wage a battle against how Roe v. Wade had changed the law of the land, and to provoke outrage at the Supreme Court. The reiteration of heated ideological conflict has been refracted and recast in important rhetorical ways as technologies of determining the presence of a heartbeat on iPhones and handhelds has offered apparent proof of the need to redetermine the medical threshold of “viability” by which expert medical testimony had established. Although the verdict of Roe v. Wade set, as it has been contested as a threshold for access to abortion, the acceptance of local jurisdictions’ ability to place hurdles before women exploited acceptance of abortion among evangelical groups to seek to restore “balance” on what was painted as an extreme decision, offering autonomy to the pregnant woman to end her pregnancy. Broad access to ultrasounds as indicators of pregnancy encourage taking cardiac activity as a line to determine the “self” of the embryo has made everyone into an expert, demoting the role of embryologic expertise in determining access to a medical procedure, recasting it as a question of medical ethics–raised as early as the Hippocratic Oath–with the passionate intensity of personal convictions.
In ways that have shifted the balance from the law of the land to public opinion–involving everyone from town councils to state legislators to take a stance on legal precedent–almost seems to have been enabled by how the televised hearings to confirm Supreme Court justices include an obligatory questioning of the status of Roe v. Wade as settled law have encouraged all television viewers and city councils to frame their own thresholds, as it has led many Republicans to develop abortion as a “wedge” ideological issue to divide the nation, encouraged not only by the accessibility of Apps to “detect & listen to your baby’s heartbeat,” exploiting the aural link of the unborn to a diffused technology, but mobilizing an openly authoritarian understanding of limiting access to abortion in early modern ways.
The unprecedented ‘freedom’ of removing state policies from judicial review by entrusting their enforcement to citizens, rather than the state’s District Attorney, suggests an abdication of the responsibility for enforcing a law that Chief Justice Roberts, himself a Catholic, begged the Court to “consider whether a state can avoid responsibility for its laws in such a manner.” The rise of “heartbeat bans” now launchd in a number of states suggest more of a multi-front attack on the “undue burdens” that restrictions on a woman’s right to chose before viability, challenging the Supreme Court and public opinion to determine whether they place “undue burdens” on women.

All were limited by state court actions, designed to exploit a roadblock placed between women and abortion rights. The restrictions on reproductive health recasts the procedure as compromising the “rights” of the unborn. The series of unprecedented legal rulings and state bills have served to restrict women’s rights to abortion, and curtail rights in favor of the unborn-effectively overturning the right to abort a pregnancy before “viability” outside the womb at twenty to twenty-two weeks.
The struggle against the practice of abortion has become one against science and medicine, or medical expertise, in the Trump administration, as most American women of child-bearing age lived in states that had adopted restrictions in conflict with medical science, but the intensity of this opposition to scientific evidence increasingly became Texas, whose governor consolidated his popularity as he endorsed the hope of abolishing abortion outright in the state, banning doctors of pregnant women to “knowingly perform or induce an abortion” and then declaring the “aiding and abetting of abortion” to be a felony, while clarifying in false faith that those who undergo the procedure are not liable.

The calling into question of what is an “undue burden” is a response to the new composition of the court which Alito is a pivotal figure, as a Catholic jurist. The confirmation since 1992 that government can create laws that restrict a woman’s right to abort before fetal viability have been distorted and expanded in the past thirty years, in order to permit the state to redefine public health access and deny women the most personal choice of whether they which to bear a child. The bevy of new cases that seem designed to put on the front burner state legislatures’ rights to erode fetal “viability” from twenty to twenty-five weeks–replacing that threshold with new standards from six weeks to fifteen weeks, or two months before viability-suggests dangerous elasticity of balancing a “burden” against state legislators’ ability,
4. The decision to allow the law to stand, both by the Supreme Court’s September 1 ruling, a decision issued without legal argument, a week before Mexico’s Supreme Court ruled criminalization of abortion to be unconstitutional across the border, and an Appeals Court allowed the Heartbeat Law Texas’ Governor signed to take effect. The “heartbeat” legislation that claims to detect the flutter of cardiac activity to warrant legal protections is both a compromising of women’s long recognized rights, and jeopardizes the well-being of pregnant women by placing the body–as revealed by a mandated ultrasound, before the heart’s chambers are even formed–above a rationality of the mind. The outsized discrepancy of using the visualization tools that allow an ultrasound to register cardiac activity when a woman might not even be conscious of pregnancy suggests an eery surveillance of the womb, even if it is presented as part of a discourse on unborn “rights,” as if these rights were entrusted to elected representatives, rather than the rights of the citizens they were entrusted to represent.
At least twelve states’ courts have imposed restrictions or requirements before women can obtain an abortion, judged not “burdens” but that effectively have weakened the “undue burdens” felt by women.

Long before the mother can sense the heartbeat–or the heartbeat can be sensed by the human ear–the ultrasound has provided a powerful new metric for anti-abortion activists to restrict access to abortion. In marginalizing or bracketing of medical science from the “legality” of an abortion, the reading of the “sacred rights” of the constitution as extending to every “person”–rather than to all citizens–given that these persons are “endowed by their Creator with certain unalienable rights, . . . among these . . . life.” Such “sacred rights” extend, in an oddly authoritarian reading of the law, in a modern misreading of a credo of the Enlightenment, to “life” such as it is within the womb, but registered by ultrasound. The law invites and rewards anyone not a state or government employee to sue anyone performing, inducing, aiding, or abetting an abortion after a heartbeat has been detected, treating “fetal endangerment” to a form of felony–seeing “life” as the first fits and hints of detected cardiac activity. The abandonment of medical judgement or ethics in such a new technology of good government that both aggressively and regressively remaps access to abortion in ways dangerous to our society and collective well-being.

