
15. While that was true before than red the reported cases of infection spread from coast to coast, tallies seemed so low in some states as pure numbers–a few states’ official tallies reported but one!–that stay-at-home orders seemed ridiculous impositions on entire populations, economies, or across huge, agrarian tracts of land. But the problem of limiting exposure to SARS-CoV-2 load, and degree of exposure to the virus able to live in aerosolized form for up to three hours, suggest no personal contact or even proximity is necessary for transmission.
By late March, barely masked frustration and rage reduced the respected Swiss oncologist Dr. Pascal Meier to juvenile taunts from elementary school as infections soar in Switzerland and the United States, railing against “covidiots” for hoarding food, refusing to don masks, or taking protective measures, revealing concern only for themselves and betraying ignorance of the pathogenic properties of the novel coronavirus and its transmission.
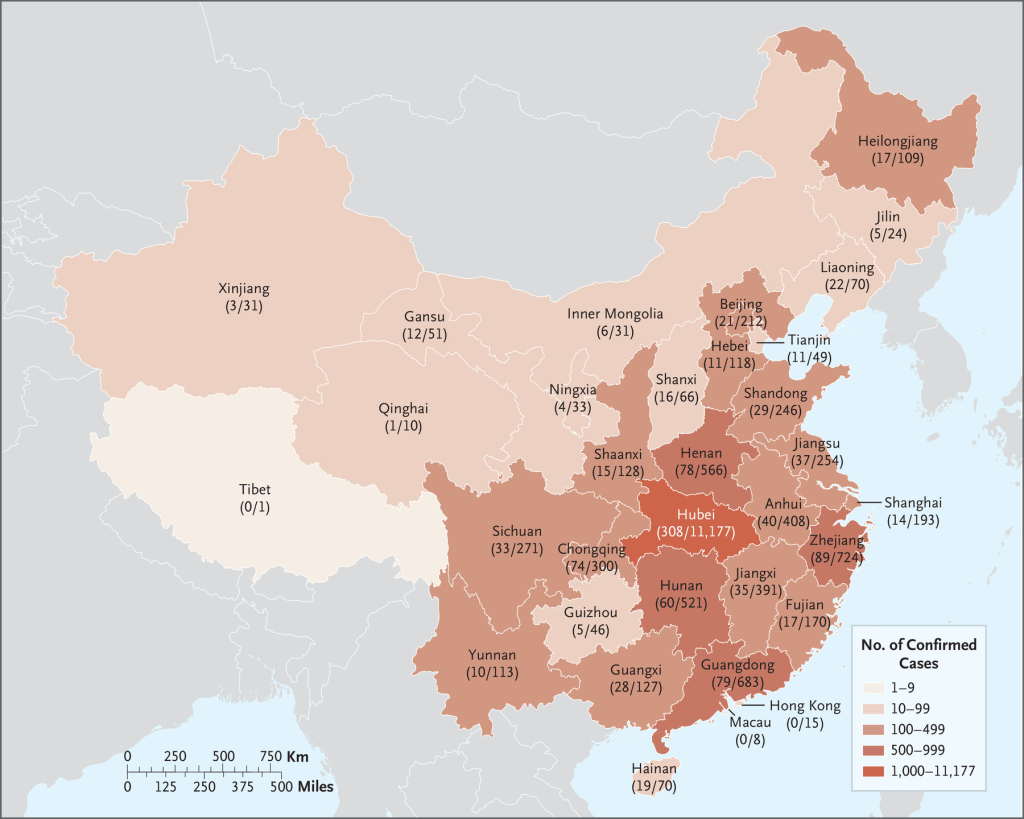
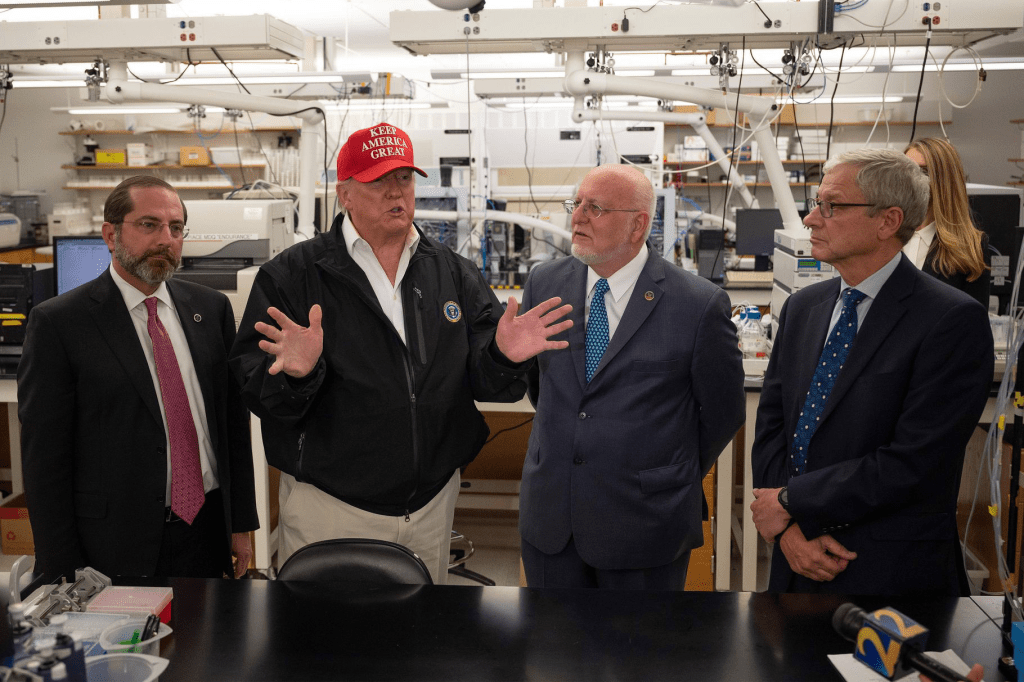
Meier’s target-in-chief was perhaps more than evident. We can only see the concealing of ignorance with a smokescreen in the eagerness of Trump showed after his initial trips to Contagious for Disease Control in early March, two months after receiving urgent warnings form the World Health Organization of the virulence of the virus raging across China, and a month after its progress was terrifyingly mapped from available data the significant ability of the pathogen to be shed after contracted–even as cases of the virus were confirmed in over nine states, and most were without the ability for in-state testing. Chinese authorities administered COVID-19 in all provinces, confirming cases in each save the minuscule sample tested in Tibet.
New England Journal of Medicine
Trump seemed to have symbolically and intellectually partitioned the spread of infection from the Homeland. His March 6 visit to the Center for Disease Control led a stream of lies to the nation that tests were “perfect” and would be immediately available for “anybody that needs a test,” and, while no public safety preparations for the virus had been taken, the assurance that in the course of the meeting, “Every one of these doctors say, ‘How do you know so much about this?” offering a specious eugenic argument about how he acquired such preternatural prognostic abilities and skills of public health, as if it ran in his family from his “super genius” uncle. His advisors were not impressed.
In many states–Montana, New Mexico; Oklahoma; Wyoming–a top-down issuing of stay-at-home orders seemed hard for governors to wrap their heads around, especially in the politicized nature of discourse about the virus’ spread and danger. President Trump championed measures that he had taken that restrained the greater outbreak of disease, and blamed his opponents for exaggerating its danger, that rendered political debate toxically muddy. For epidemiological realities warranted far greater emergency measures than a regular set of public addresses assuring future promises, and testing: instead, we have the website Oscar, modeled after Alexa, promoted by an insurance company closely tied to the family of son-in-law Jared Kushner, who seems keen to use inside information about the virus’ danger to turn a profit.
The dangers of transmission and the effectiveness of social distancing of six feet were quite intensely debated in the medical community: the six feet rule that CDC issued looked reasonable, as a guide but airborne transmission from sneezes, aerosolization, and the virus endures in aerosolized form for up to three hours. It seems almost impossible to predict the load of the novel coronavirus one would be exposed by a simple map of mortality, let alone compromised public records conducted with limited testing and no testing for antibodies or exposure to viral load.
15. The outbreak had by March 10 just barely begun, but no stay-at-home order were in place. The six counties in the Bay Area, from San Jose to Marin, who issued the first shelter-in-place order–Alameda, Contra Costa, Marin, San Francisco, San Mateo, and Santa Clara counties–on March 17, 2020, restricted all non-essential activity, and was extended in early April to May, followed the absence of national directives in Trump’s largely self-congratulatory address to the nation, of May 13, whose stunning absence of enacting preventive measures seemed to punt in response to the declaration that day of a global pandemic. Although incomplete testing data was not yet fully compiled, and tracking of COVID-19 in the states was woefully incomplete. Testing for COVID-19 unavailable in multiple states; the absence of testing, and the urgent need for its expansion by many, including Bill Gates, who first began to call for collecting specimens inadvertently describe as “home testing kits” before Trump’s speech, in an era when Seattle was an epicenter of the virus’ spread, and the sudden rise of COVID-19 in Washington counties suggested a rapidly rising curve and immediate need for further testing.
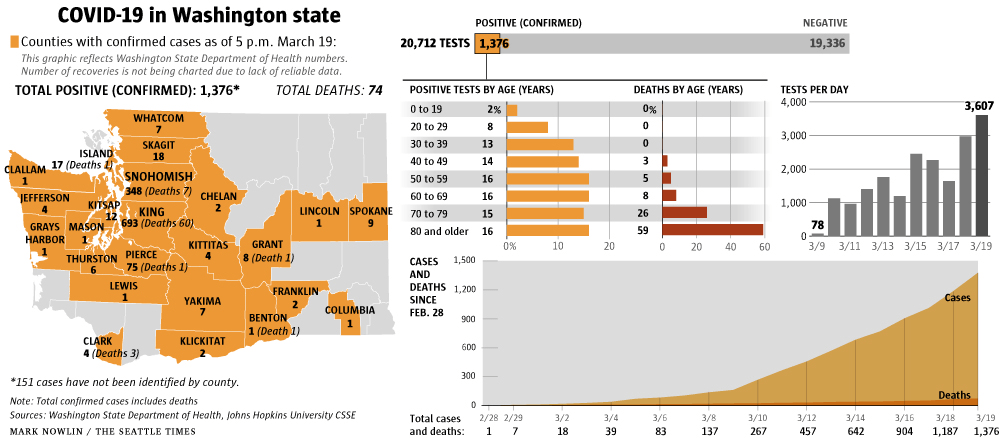
A continued absence of national data–and reliance on state databases–emphasized the gap between national oversight of a much reduced CDC agency, and a lack of national oversight that foundations, corporations, and other entities tired to remedy with desperation by stepping into the breach. If the first cases of COVID-19 were evident in Seattle in mid-February, sending alarms through contagious diseases laboratories, with Microsoft employees reporting infection by the illness on March 4, and two other cases at Facebook, Microsoft instructed employees to work from home, setting a precedent for Shelter in Place acts. As the spread of the disease by late March had blossomed into a pandemic, by March 25 local radio stations announced they would no longer take time to broadcast Trump’s daily address, due to misleading information unable to be verified in real time, accentuating the region’s split from the Presidency, and the deepening levesl of public distrust.
Gates’ calls were amplified as Shelter-in-Place orders went into effect, and the Gates Foundation begun computational modeling of viral spread. The contrast of this attempt to mobilize to the benign neglect the Trump administration practiced in recent months of reassurances combined with an offloading of responsibility to regional governors seems driven to the uneasy or unproductive relations of many to the President, whose personalization of the crisis is refracted through partisan conflicts. Indeed, Gates’ frequent warning of the dangers of a pandemic that was global has been elided with the global conspiracy theorists who find the global scope of coronavirus COVID-19 the site to spin global theories: Gates is not Jewish, but fits the bill of a global plot orchestrated by a diabolic puppeteer, from George Soros to Bill Gates to China, as the world is possessed of a lack of security, and the fear that Gates had imagined a pandemic spread from China as proof of his tie to the virus: yet the fears Gates voiced were grounded in the past outbreak of avian flu epidemics and outbreaks of African Swine Flu in China–
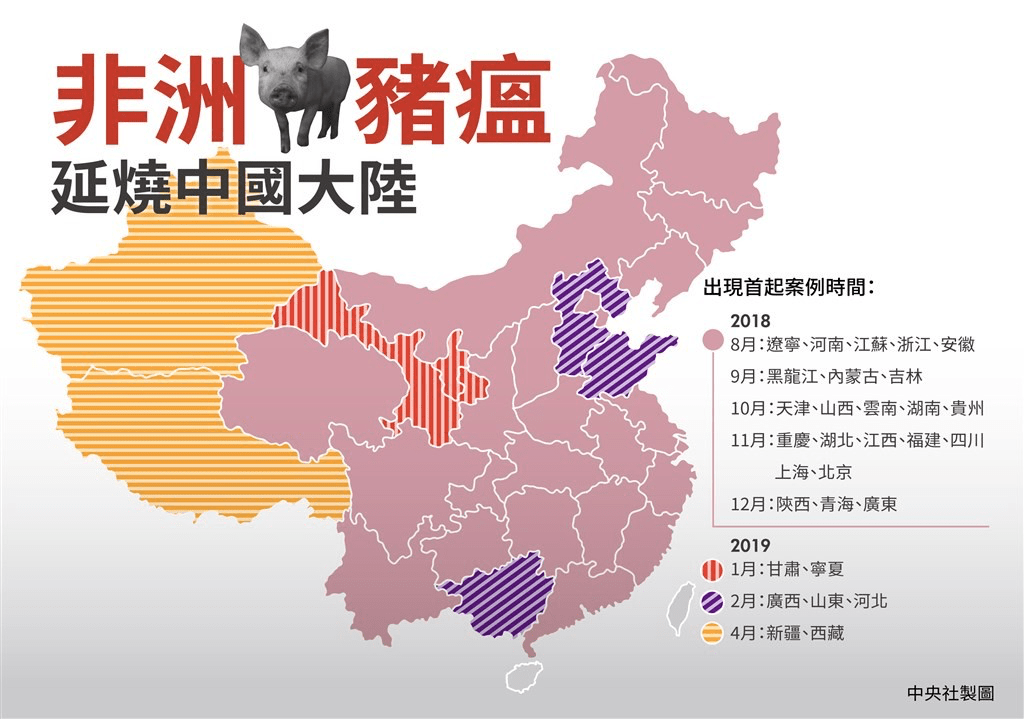
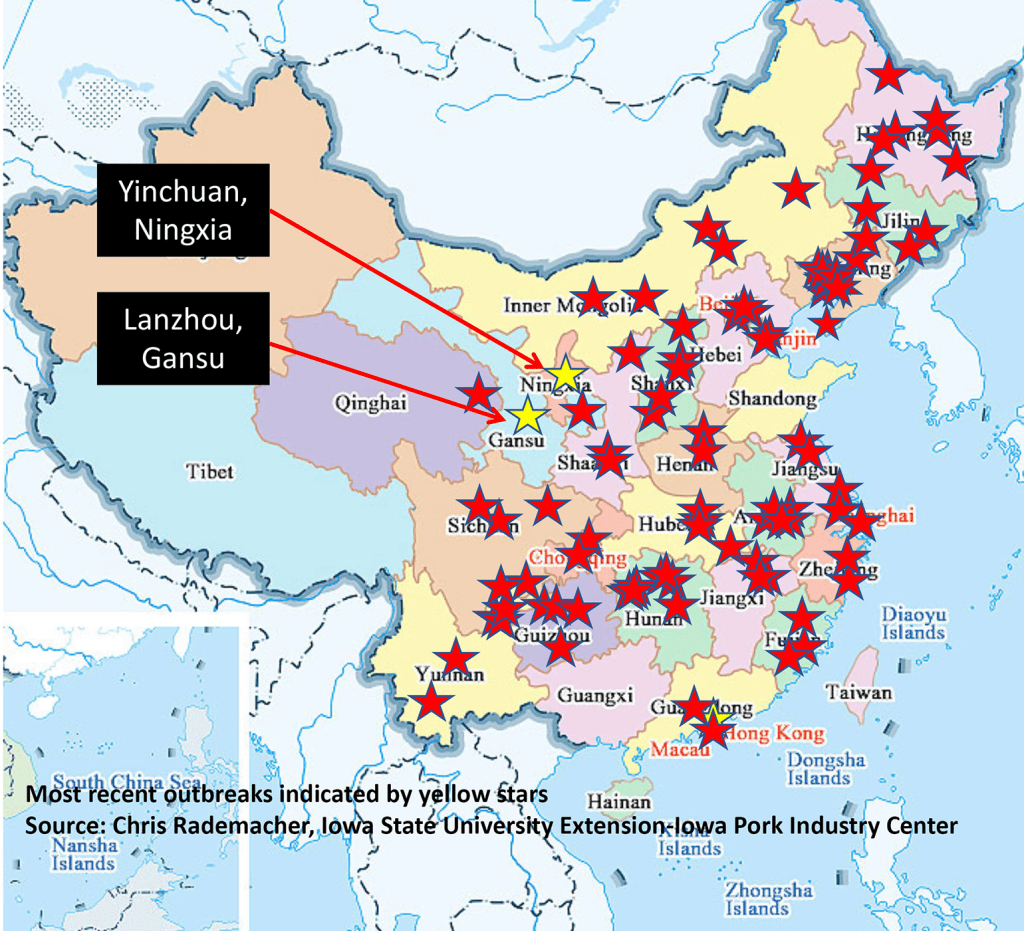
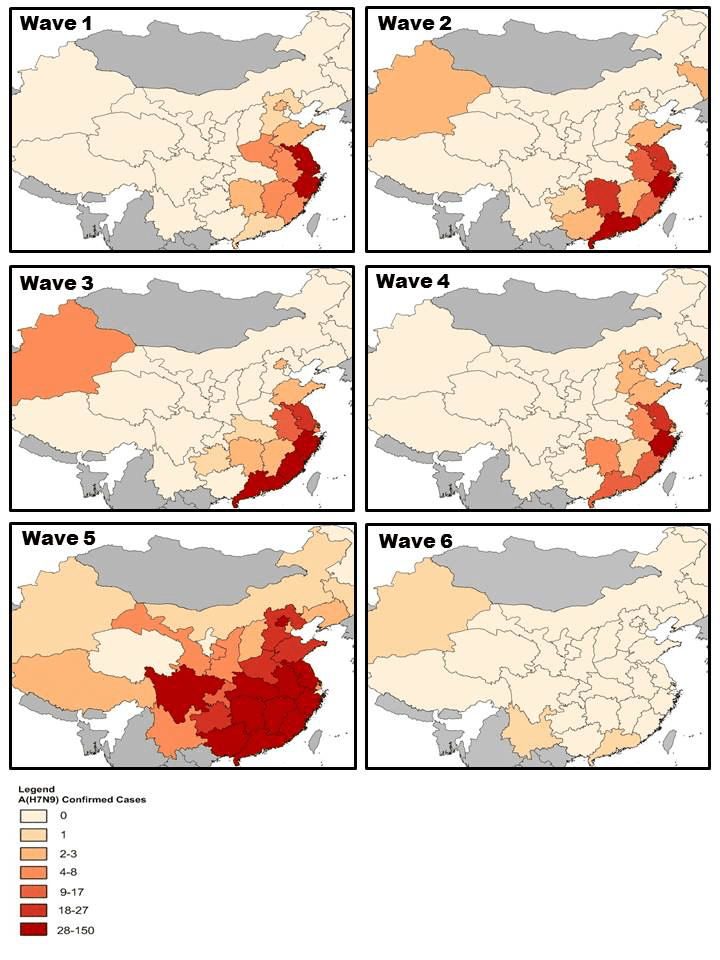
–and other waves of zoonotic pathogens, from avian influenzas that have ben transmitted to humans, often from infected poultry, from H1N1 to the feared H5N1 to H7N9, to H10N8, as the fears of contamination from meat sources have escalated in recent years. “Don’t touch live poultry!” has been a common foreign advisory in Chinese markets, as diseases are increasingly jumping from animals to humans, who lack antibodies or protection or vaccines, as influenza strains have proliferated as bird flu strains previously confined to China have led to human fatalities.
The image of diseases from Asia cannot be dismissed as a topos of literary origin that descends through Dostoevky’s Raskolnikov’s apocalyptic vision that “dreamed that the whole world was condemned to a terrible new strange plague that had come to Europe from the depths of Asia,” as one that “epidemics always came from the darkest recesses of the East”: when they are quite open to view, there are indeed a group of viruses whose spread is mapped from China,–decidedly are not “Chinese” in origin.
The Asiatic origins of Cholera were so widespread that the name, Asiatic Cholera, was the prevalent descriptor of the infection whose profile had not been seen before, or the ravages that it ssemed to perform on the human body. The foreign nature of the disease is an externalization of it, all the more important as we are not able to map it effectively within our own space, as it remains unknown: and the resurgence of the descriptor of the coronavirus as a virus manufactured in “Chinese viral labs” in Wuhan, for which there is no evidence, seems the latest version of the projection of foreign identity upon a plague, much as the arrival of venereal diseases was imagined to be the arrival from a foreign nation–the “Mal francese” or “French disease’ in Italy, the “Italian disease” in France, the “Christian disease’ for Islam, and, increasingly, the disease of the New World. Has Trump & Co. assigned the disease to a Chinese labs, to conceal the major cuts they made to any scientific cooperation on antimalarials and viral pathogens with Chinese disease centers from 2018, a slight change from blaming “Chinese secrecy” as manipulating the World Health Organization?

16. It is not that the contagious virus spread was imagined as having occurred along a red-state/blue-state divide. The regions that were most exposed to the arrival of viral strains, from the Bay Area to Seattle to New York to Orange County were sites where the virus indeed first arrived from China, long before early February travel restrictions: but the shores where population was most congested, personal spaces overlapped the greatest, health care sites and hopitals are focussed, and aging populations are most densely congregated, became sites where confirmed cases of infection were registered, leaving much of the “heartland” of the nation unaffected. Did such maps help assist cure theorists that tied the virus to globalism, imagining that characterized the relation of Bill Gates and his Foundation to “the creation and spread of this virus” was in fact “open for investigation,” as the virus from China mutated on social media networks if it had not yet actually mutated.
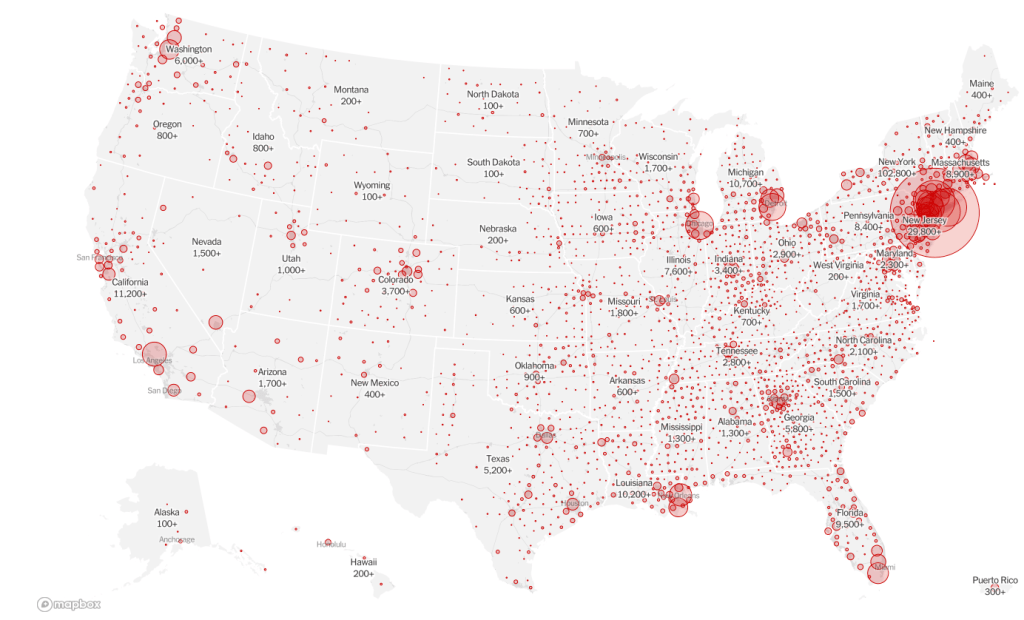
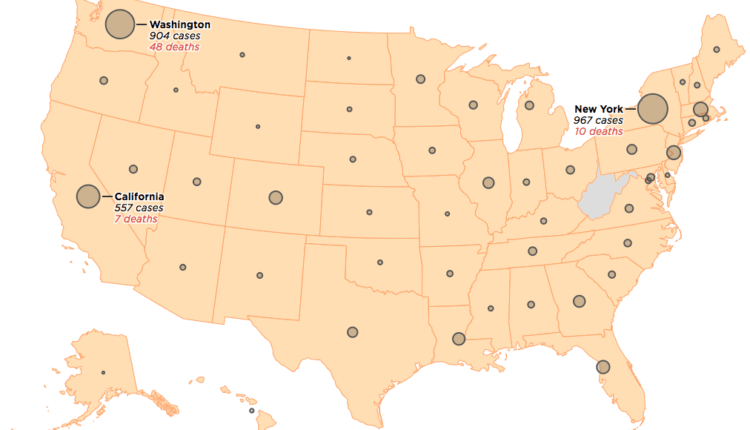
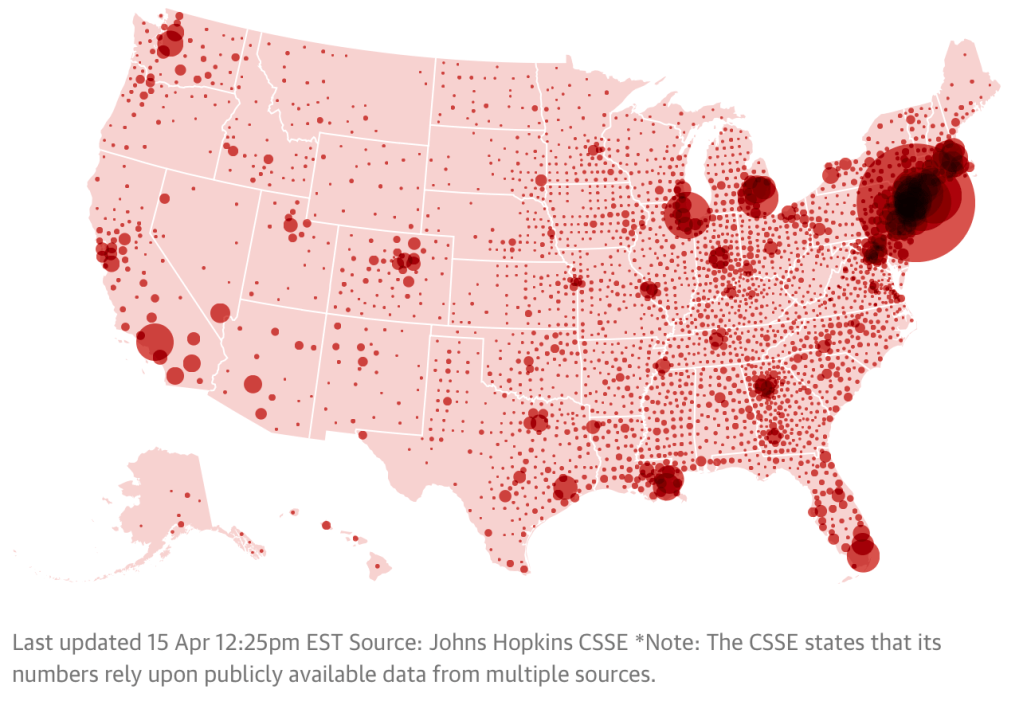
And even as cases in almost all the states in the union were evident by the end of the month, we focussed unduly on “hot-spots” like New York, and counted our stars we were lucky not to live there–or closed the entrances to other states to those darned New Yorkers, who maybe got what they hadn’t prepared for adequately–and the notion of a national policy seemed distant and, well, un-American in a land of personal liberty. As Microsoft news–to which Gates has no current tie at all–predicted the coming fears of the spread of COVID-19, regularly growing by eight points a week, by late March. The notion of “hotspots” that circulated in the news, as if to suggest where the front lines were on a war, was quickly replaced by late March by a dot density maps from Mapbox, that suggested the distribution as a temporal progression, taking the temperature of the nation, effectively, by the density of ever-growing red dots that redefined each place in the nation, substituting the centrally meaningful index of cases of infection reported from all else. Dots shifted their layers of intensity or correspondence to buckets, as they ineluctably grew.

What was a truly critical moment demanded consensus to frame a workable national health policy. Was this a deep cartographic failure, as much as a lack of good data about the spread of infection, and accurate tallies of patients able to test positive for COVID-19? The problem was not in statistical modeling; the absence of good counts of positive cases of infection in our nation–or probably of verifiable and trusted tallies of infection rates in China, where the virus first spread–created deep misconceptions about the flow and transmission of the virus COVID-19, which later apps tracking the progression of the virus in the nation would only later redress.
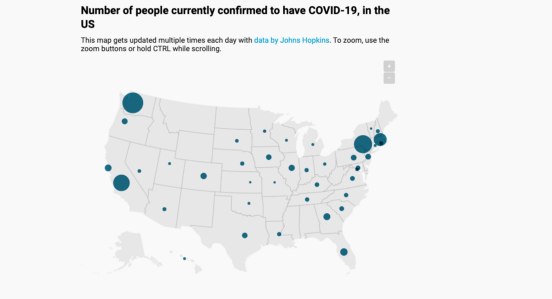
When we turned to describe “centers of infection,” the result was almost comical at the end of the month, as the meaningful nature of a “hot spot” disappeared in a sea of melancholy blue.
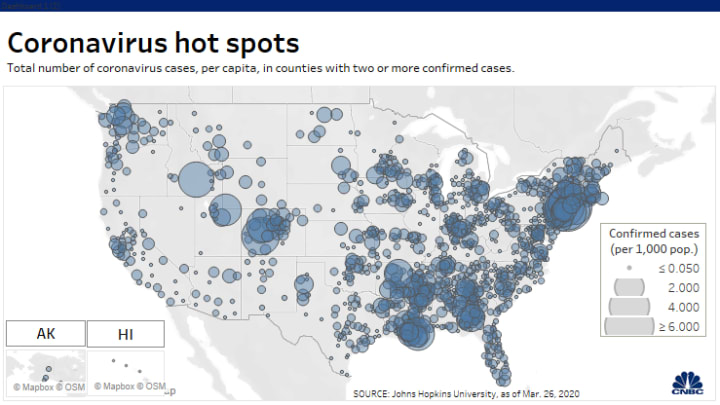
CDC, followed by others, mapped the spread of disease in a disembodied way, as if to reveal grasp over its geographic spread by choropleths that shaded statistics across areas, rather than in terms of human subjects. The consequent distribution of aggregates that didn’t track the virus but rather the manifestation of symptoms, without communicating the incubation or virulent transmission of the virus, and often used buffers to individual cases, independent of population density or increased probability of infection: it seemed that as we mapped the symptoms of the nation, rather than the multiplication and pathways of what were clearly local epidemics, each of their own course, and their own relation to shelter-in-place policies, that we were distancing ourselves from the global scope of the infection, or even from an epidemiological portrait: t he data itself was limited, quite uneven across the state, and not even accurate as a progressive illustration of numbers of cases.
The Center for Contagious Diseases, relying on diverging local tallies of verifiable cases, created meaningless aggregates of states, as if this were an electoral map–even as individual attorneys general issued stern warnings states about misleading advertisements for products marketed as COVID-19 “cures” from chlorine dioxide, hydroxychlorquine, essential oils, and garlic–echoing spiritualists’ claims in South Asia that cow dung rendered bodies cleansed of the dangerous virus. CDC national maps suggested little sense of alarm outside the coastal states by March 12–
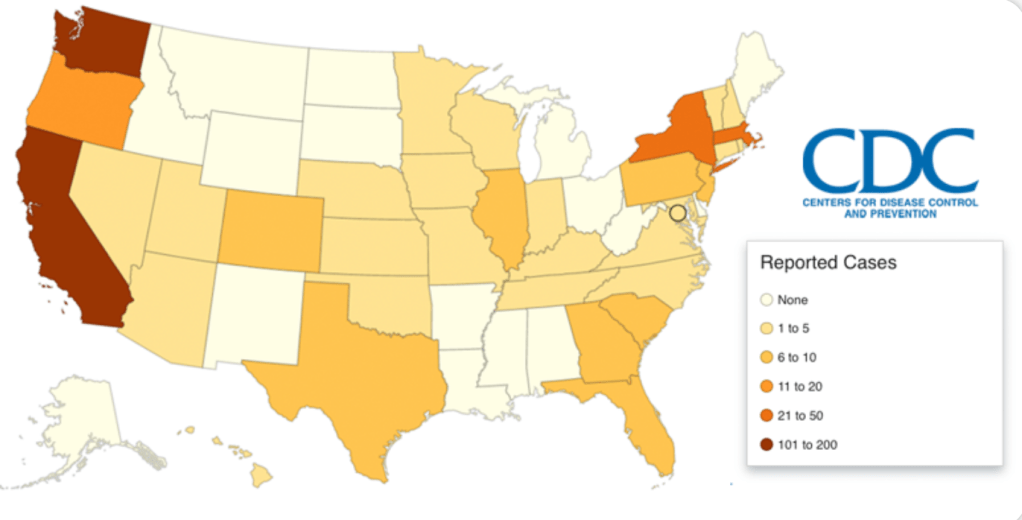
–and even as Trump defined a “national emergency” in response to the identification of a “global pandemic,” on March 13, low “reported cases” still suggested that states were able to contain a problem that clearly spread across space in ways we didn’t fully understand–without counts for multiple states, even quite late in the COVID-19 game.

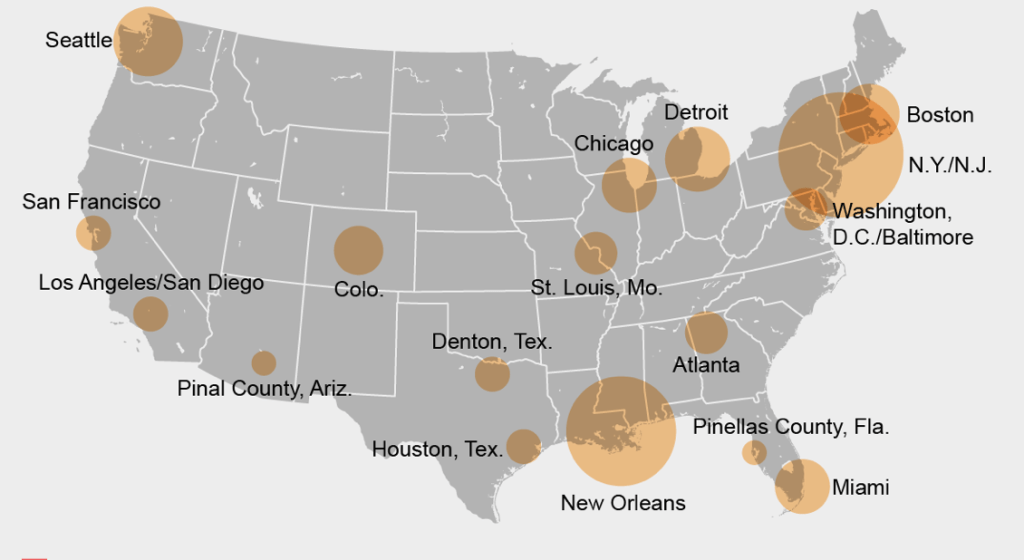
And by March 19, COVID-19 cases were growing at a record of 500 a day, as cars lined up over two miles to be tested in the rare drive-thru testing center, sending many regional health professionals into panic mode, but we looked to maps for a sense of relief, in our fragmented United States, believing that hot spots lay somewhere else, at a safe remove, even as hospitals entered periods of stressful overloads, shortages of needed masks and preventive equipment, and health care workers faced increased duress. If the number of such “hot-spots” had shifted over much of the large urban areas of the east, by late March, the discourse of uncovering further “hot-spots” continued as a debate of data analytics, balancing counts based on total confirmed cases of infection with the uncovering of “hidden hot-spots” in smaller population centers, often obscured by the greater numbers found in larger population centers.
Center for Spatial Data Science, University of Chicago

Amanda Montañez/ Marynia Kolak, Xun Li and Qinyun Lin Center for Spatial Data Science, University of Chicago

Yet from early April, it made sense to paint the entire nation pink even in a choropleth, and that the density of some centers of population were simply drowning in cases of the contraction of the virus in ways that mandated more medical supplies, as we faced new prospects of shortages and insufficiencies more commonly associated with healthscapes of other countries. The globalization of the disease and, in other words, created an eery sense of the equalization of the map and shortages of not only ventilators, but masks, gloves and sanitary equipment, face shields, and food that we rarely imagined would arrive just two months ago.


Pingback: Our Unclear Path Forward: Contagion Advances | Musings on Maps