
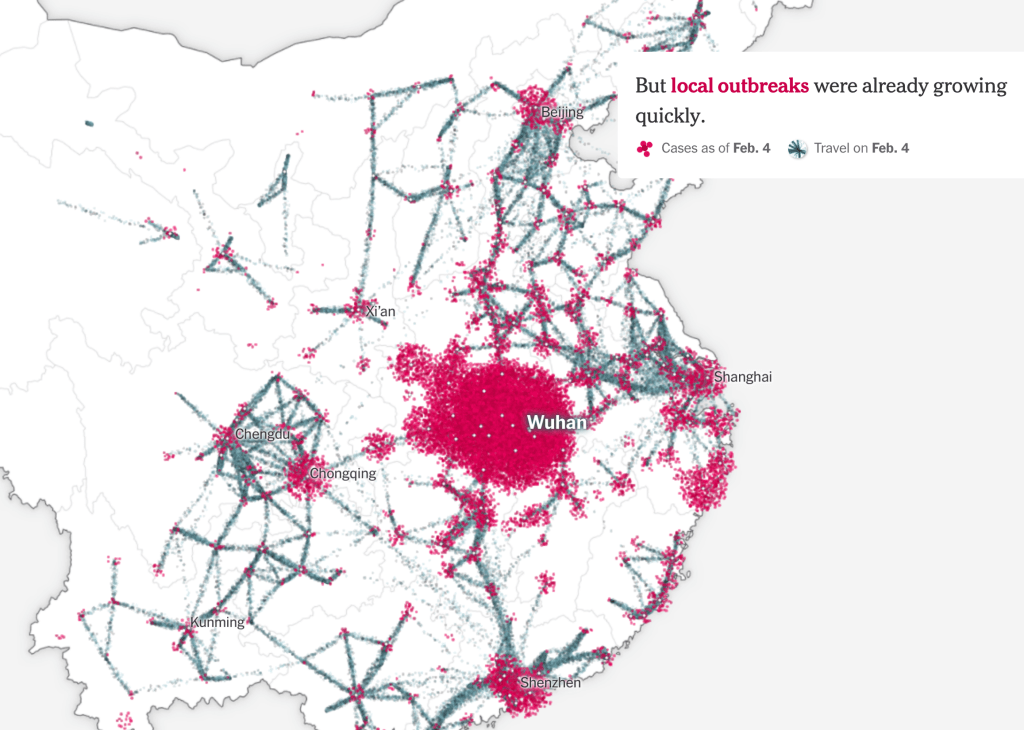
A pandemic is by its nature both local and global by definition–and begins from a local outbreak. But if the only way to gain orientation to a pandemic is by accurate local counts, the problem of balancing–or toggling between–the local and global has become staggeringly pronounced in the case of COVID-19, as if the point-based cartography that we use to track the disease has the better of us, and upper hand, with the absence of accurate local counts. The lack of clear data that came from Wuhan in the days that followed the outbreak of the virus revealed worrisome problems of transparency. The difficulties Chinese government authorities faced in getting bearings on the zoonotic virus, lab-born or not, raised problems of even trying to map its rise, and we tired to look at maps as tea-leaves of future responses, as well as retrospective diagnoses of the point of origin of disease spread–as if maps could explicate our uncertain conditions, and increased vulnerability.
Data visualizations since seem to proliferate in response to uncertainty and an absence of consensus, as we turned to maps as a hope for truth in an age of increased uncertainty: as local officials were loathe to shoulder responsibility, the tally of infected in Hubei Province jumped, astoundingly, forcing the government to recognize the ease of its transmission among humans, was far more virulent than believed. But at this point, looking back in the mirror provides little sense of orientation to the multiplication of dispersed local outbreaks of coronavirus that we are increasingly challenged to map in relation to ourselves. Were the first maps of the New World similar responses to the deep sense of religious and eschatological uncertainty of the early modern period? Whether or not that was the case, we all felt especially early modern now, plague victims of a sort that led us to look back on the mapping and mapping of responses to the spread of pestilence, and hoping that past experience–or our current increased ability of empathy–gave us more meaningful access to the epidemics and pandemics of the past.
The sudden uptick of cases reveals a reticence in tallying the infected out of fears of reprisals for apparent incompetence, an institutional blame-shifting triggering mechanisms of concealment that has led American meat-packing plants to hide numbers of infected workers, and numbers of tests for infection to be far lower than official records suggest: the absence of ability to control the spread of SARS-CoV-2 led us to proliferate maps in hopes to grasp its rapid doubling, uncomfortable at the world they began to show, apprehensive at how to come to terms with the rapidity of local outbreaks of confirmed cases with sufficient granularity, and enough continuities, hoping to track contagion as hopes of containment were beginning to fade in the new aggregates that were increasingly evident.
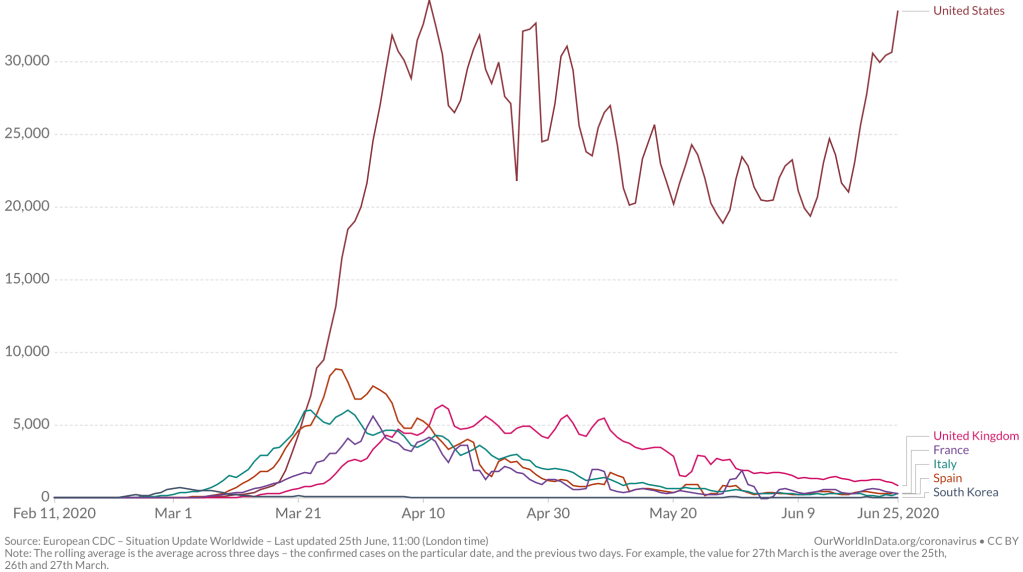
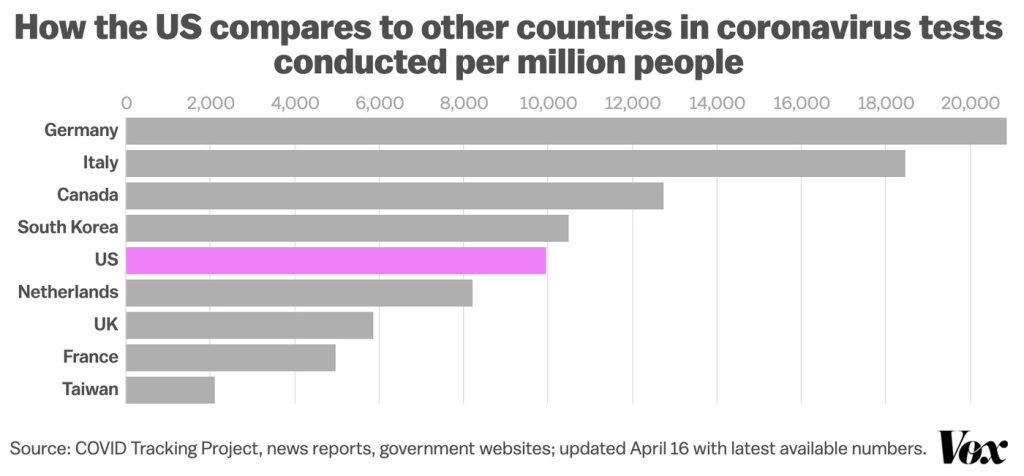
The warning of the virus’ spread was raised by Li Wenliang on December 30 from Wuhan, inter-agency shifting of blame and responsibility in Wuhan– a reflexive institutional blame-shifting by “throwing woks”–abruptly ceased with summons of Shanghai Mayor Ying Yong, he who lured Elon Musk to Shanghai, to restore order: as a new hospital was built, tallies of new cases of coronavirus in Hubei astronomically grew by nine from 1,638 to 14,840, shocking the world–a figure was in keeping with the nearly 1,400 people dead in the country, but suggesting a viral load of unprecedented proportions. Americans apprehensively watched the disease afflicting passengers of cruise liners as if it would arrive ashore, its virulence was in fact already of pandemic proportions: yet American disinformation here took over, as we were told to stick our heads in the sand, ostrich-like, as fears were overblown, and tried to keep calm. And then, the tables were turned, as the United States President described, or suggested, a national policy of intentional undercounts, and limited testing, lest the counts discovered tank his popularity–the stock market value of Trump, International, or, rather, Trump-in-Office, Trump-as-Chief-Executive, whose new season might be canceled due to low ratings. And although the virus began in China, how the United States increasingly came to be the outlier in the numbers of infection confirmed weekly suggested a national story of mismanagement, as the narrative we told ourselves of American exceptionalism before illness seemed to have boomeranged, with the three-day averages of confirmed infections skyrocketing, and setting us apart from the very nations we compare ourselves to, but whose health-care policy we increasingly realize we are distinct from.
Americans were soothed by deceptive common-sense talk. But the results of a lack of investment in public health are all too evident, if our maps are . Robert Redfield, a virologist who served as the public spokesperson of reassurance who had long sustained false theories about retroviruses causing HIV and AIDS, argued that even if the fourteen confirmed cases of the novel coronavirus were monitored and traced, “the virus more exploded . . beyond public health capacity,” he seemed to forget he had not developed that capacity. Virology is of course Dr. Redfield’s area of expertise, but he won his political post in no small part by being practiced in massaging truth statements for political ends. During AIDS outbreak, the last major plague in the United States, he had advocated unproven drugs billed as HIV vaccines and encouraged quarantine, abstinence, and stripping the medical licenses of HIV-infected medical workers, more than accelerating cures; Redfield took time to blame the Obama administration for implementing clinical tests, to please his patron. Bt he obscured the level of infections that in truth were not known, blinding the nation to a cartography of COVID by not advancing adequate levels of testing, that returned us to the simple equation of the dog days of AIDS, only able to make us yell, yet again, this time with Larry Kramer, stalwart resistor of the silencing of AIDS by the failure to use on-trial medicine–
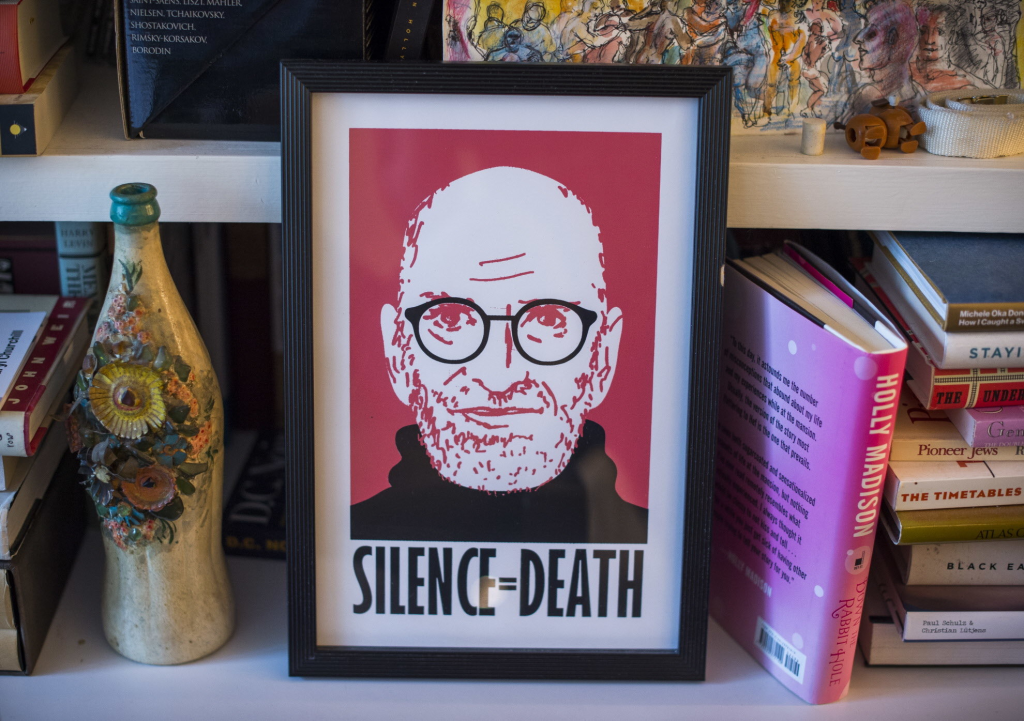
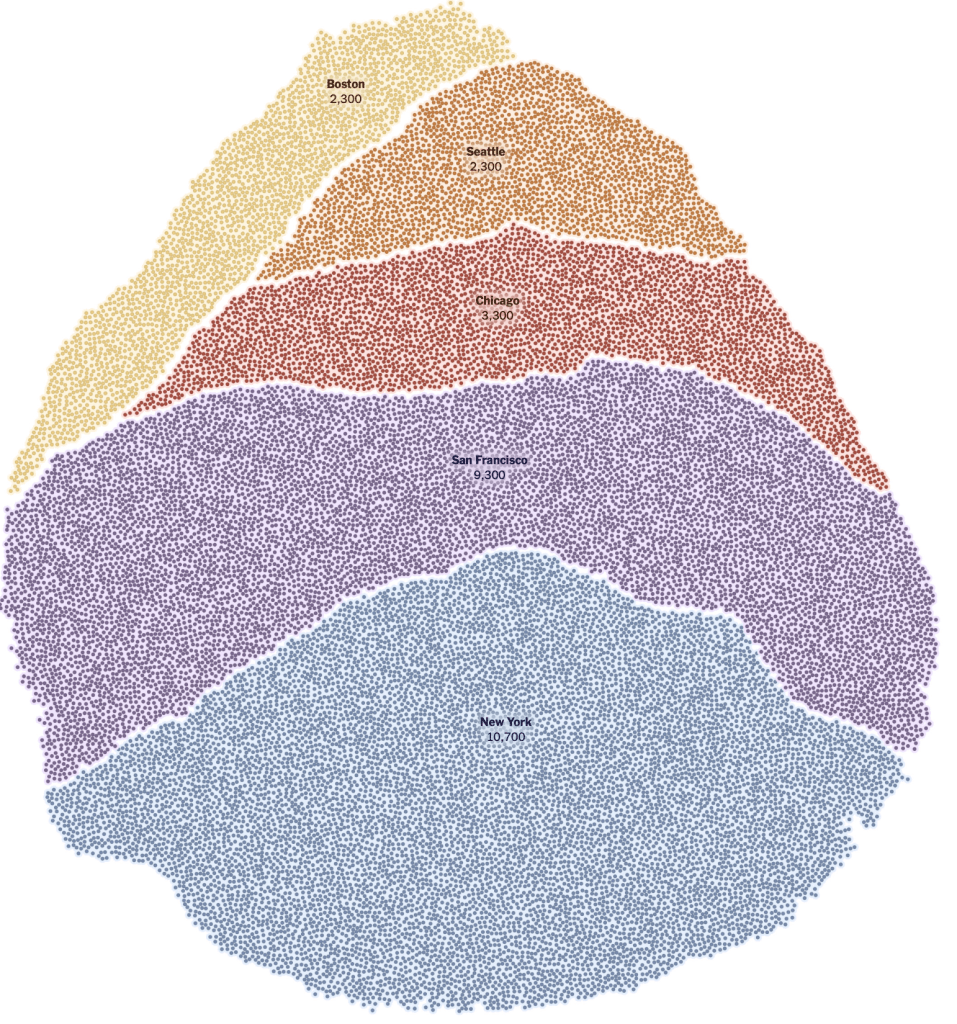
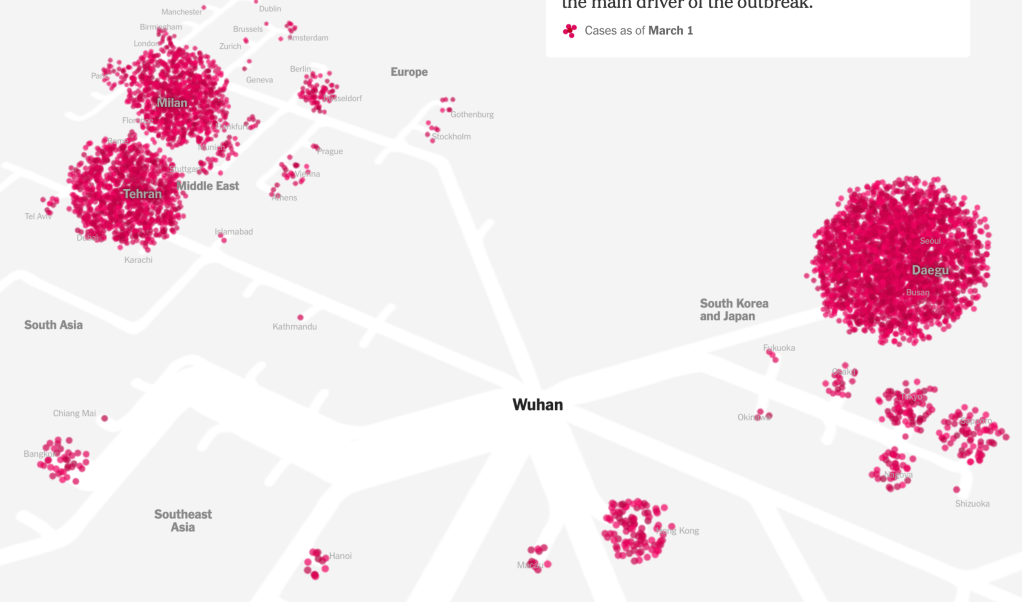
–at the utter deception with which we met the pandemic. Dr. Redfield must have met his commission to radiate calm by assuring Americans in late February. As he assured us only fourteen cases had been diagnosed in the United States, the number meant little, as any virologist should kmow; while hindsight is a benefit that obscures us from the need to life life forwards, we suspect urban hotspots were already laden with infected individuals by March 1, a silent ticking bomb of urban outbreaks already infecting 28,000 as it spread broadly its “hotspots”–New York, Chicago, San Francisco, Seattle, Boston and Chicago–all of massively different density, without tests being able to affirm the scale of its spread.
There was no map. And then, all of a sudden, the globalization of coronavirus hit home; any place in the world could be related to any other place, as rates of infection bloomed globally in geographically disjointed hotspots, spatially removed from one another, even as a standard for uniform testing lacked. And there was no sense of an art of dying, as the amazingly rapid contraction and worsening of illnesses left many without a script, and many more silent before a dizzying multiplication of statistics of mortality in the face of COVID-19, several weeks later.
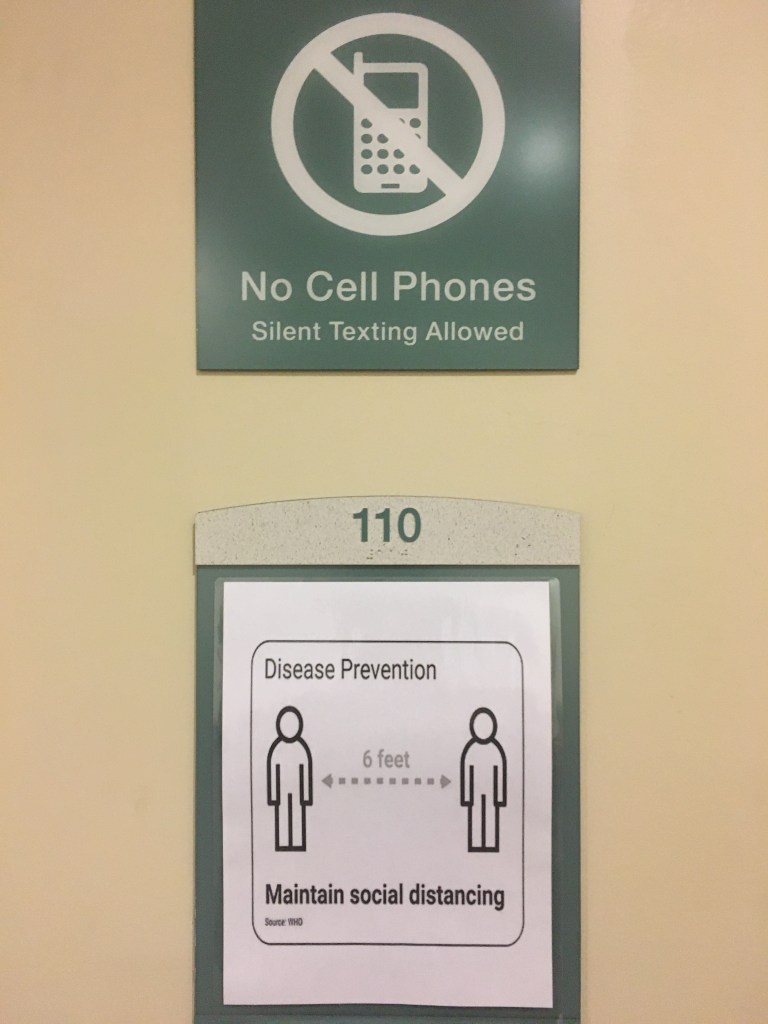
Every other map of COVID-19’s spread seems an attempt to persuade the viewer of its accuracy and totality, in retrospect, even as we have no clear sense of the total figures of infection-or even of the paths infection takes. We are mystified by the geography and spatial dynamics of the virus’ travel, but realize the severe communicability of a virus whose load is stored in the naso-laryngeal passages, and can be communicated by airborne drops. Is distancing the best way we can constrain the geographic spread of infection? Can statistics demonstrate the success of curtailing its spread?
It was a hidden agenda in the maps of news agencies and to register the accurate levels of infection, promising the sorts of transparency that had been clouded in much of January. And while we watch the progress of the pandemic on screens, there is a sense of truth-telling, as a result, of revealing the scope of the virus’ actual spread that compensates for the lack of clarity we once had. But it is also increasingly difficult to orient ourselves to the GPS-enabled scales of its spread, for we still are looking at pretty limited and almost superficial data, in the sense we have trouble plotting it in a narrative context, or find a reaction more than shock. The virus is easy in ways to personify as a threat–it wants us outside; it comes from afar; it pervades public spaces and hospital grounds; it demands vigilant hand-washing and sanitizing–but the very numbest are elusive. While we try to track reported cases, hoping that these limited datasets will provide orientation, we have been lumping numbers of tests that might be apples and oranges, and have not found a consistent manner of testing. Deaths are difficult to attribute, for some, since there are different sites where the virus might settle in our bodies.
Even while not really following the pathways of its transmission, and the microscopic scale of the progress of the pathogen in bodies. And if we rely on or expect data visualizations will present information in readily graspable terms, we rarely come to question the logics that underly them, and the logics are limited given the poor levels of global testing for COVID-19. It is frustrating that our GPS maps, which we seem able to map the world, can map numbers of surrogates for viral spread, but we have yet to find a way to read the numbers in a clear narrative, but are floored by the apparently miasmatic spread of such a highly contagious disease that makes us feel, as historian of science Lorraine Daston put it, that we are in “ground zero of empiricism,” as if we are now all in the seventeenth century, not only in being vulnerable to a disease far less dangerous or deadly than Yersina pestis, but without explanatory and diagnostic tools.
This was, to be sure, a past plague come to life, requiring new garb of masks, face-shields, and protective gear for health workers–
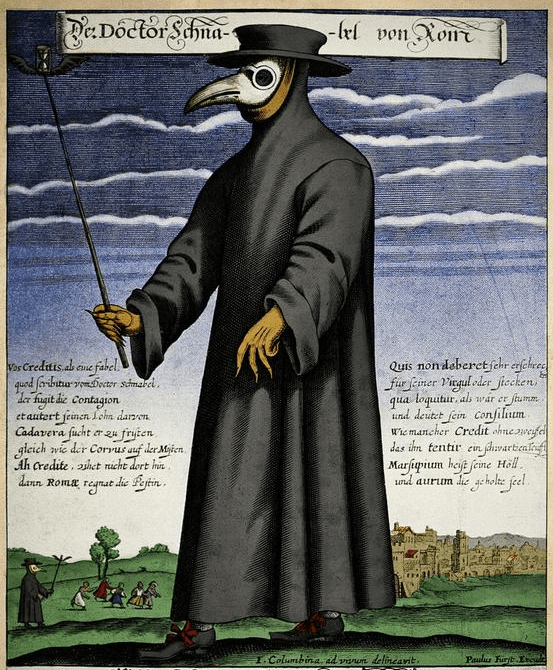
–as the cloaks, leather gloves, staffs and masks that made up early modern protective gear returned to fashion, as if in a time warp, in new form.
We find a leveling between folk remedies and modern medicine, as we live collectively in what she calls a “ground-zero moment of empiricism”–if one in which we are deluged by data, but short in knowing what is data, as we are lacking in explanatory models. This is a bit unfair, as we still can profit from autopsies, and have been able to contain spread by hand-washing–but the images of a single magic bullet, or antiviral cure, are far, far away in time. But there is no longer any familiarity with an art of dying, although we found we encountered death with an unforeseen and unpleasant rapidity: we moved from hopes for awaiting immunity or antivirals to a basic need for some consolation of our mortality. There was no possibility of transcendence in a crisis of mortality of dimensions and scope that seem outside the modern era.
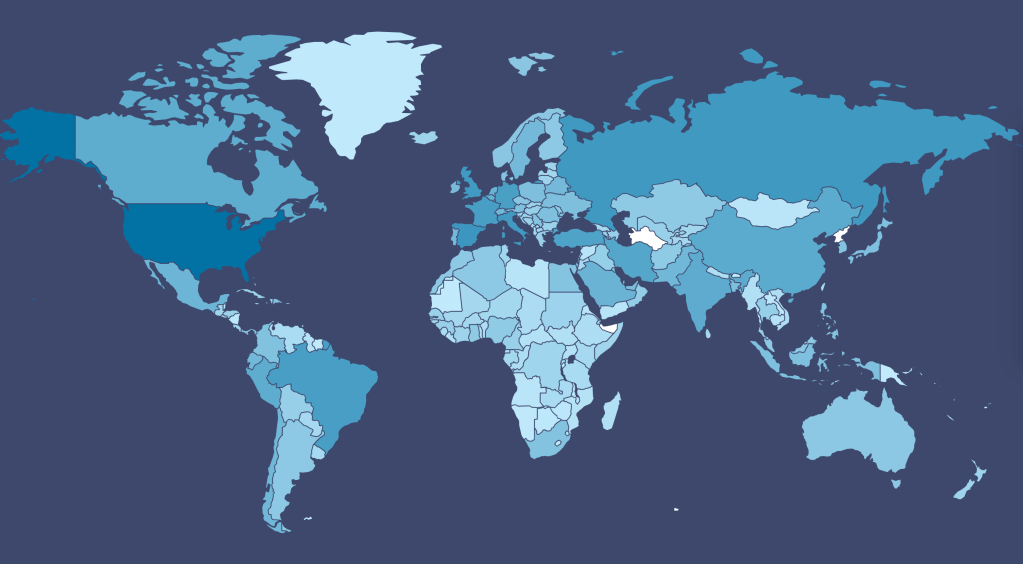
And it is ironic that distancing is the best mode to prevent infection–and many deaths may have been enabled by quicker decisions to adopt practices of distancing that could manage viral spread, Trump seemed not to notice that the very globalization he had resisted, and swung against with all his force to win votes, had facilitated the spread of a viral agent whose arrival was denied even as SARS-CoV-2 had already begun to flood the United States, in ways we only mapped in retrospect, as a global village that by March 1 had already grown satellites of viral loads in South Korea, the Middle East, Iran (Teheran), Europe (Milan; Gotheborg), South East Asia, and Hong Kong, as we anticipated its arrival with no health policy in place and no strategy for containing what was already on our shores. The global crossroads defied any choropleth, but we had only mapped the virus for some time in choropleths, as if believing by doing so we could not only map it by national boundaries to keep the virus at bay.
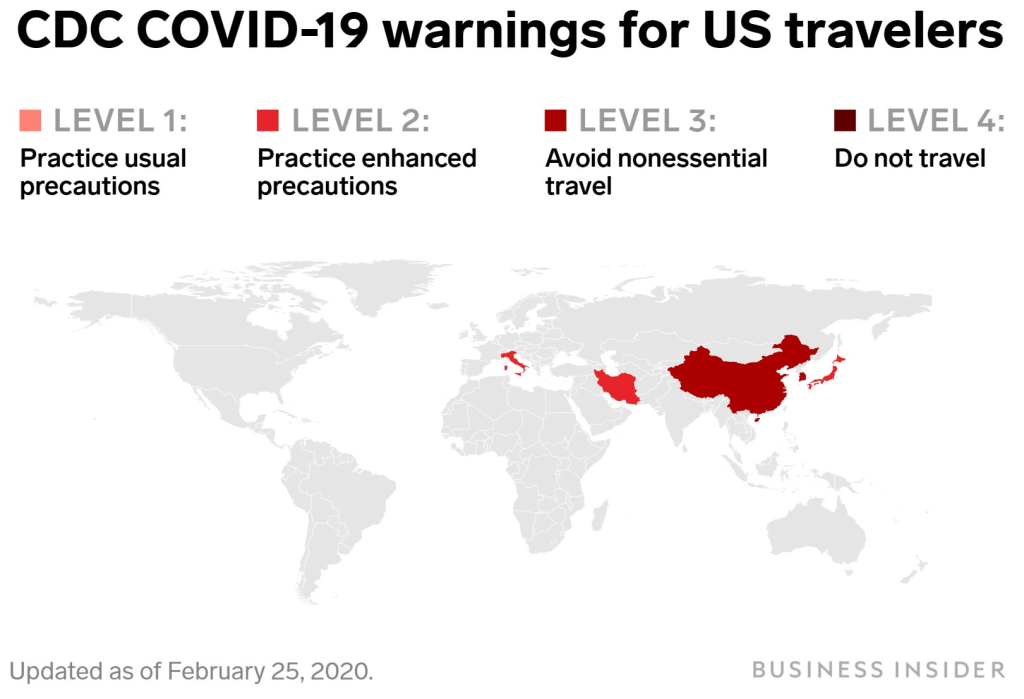
But if we lacked a model of infection and communication of COVID-19, we lacked a sense of the geography by which to understand its spread–and to map it–and also, deeply problematically, an inter-agency coordination to assess and respond to the virus’ spread as we sought to contain it: and in the United States, the absence of any coordinating public health agency has left the country in something like free-fall, a cluelessness emblematic by a map cautioning American travelers to take enhanced protections while traveling in Italy or Japan, two major destinations of travel, and avoid all nonessential travel to China, but refrained from ceasing travel plans.
1. The most compelling language of the novel coronavirus is “false positives” and “false negatives,” that seem to betray the unsure nature of standards; the most haunting is the multiple sites COVID-19 can appear in the sites of the body we use to map most disease. While we associate the virus with our respiratory tracts, the virus can do damage to multiple organ systems, as well as create blotchiness of “covid toes” due to burst peripheral blood vessels; it can damage multiple organ systems simultaneously, including the kidneys, heart, lungs, brain, and linger in our intestinal tract where it can flourish and proliferate; the virus can reduce the ability of our blood to form clots, or disable our ability to form clots. The ACE-2 receptor protein, a launching pad for viral infections, lies in our lungs and respiratory tract but in stomach, intestines, liver, kidneys, and brain. Increased sensitivities among those suffering from high blood pressure, cardiac disease, and diabetes reflect the nosological difficulties of classifying the virus as a cause of death or to grasp it as an illness, let alone to read data about the disease. If the virus lodges in the most delicate structures of the alveoli, which it causes to collapse as it infects their lining, it can take multiple pathways in the body, and as its pathway of infection may be multiple, medical response must be improvised with no playbook for clinical care.
All we know is that our medical staff desperately need protective gear. On top of that, it hardly helps that we are without a clear national policy, and find that the United States government has engaged in far less transparency that one could have ever expected.
We can only say its spread is accelerated dramatically by structures of globalization, and it stands to disrupt them. utterly Even as we map what seem total global knowledge of the disease, analogous to what we have come to expect from Global Positioning System, the multiple holes in our picture of the spread of the disease provide little sense of mastery over the pathways of communication, contraction, and infection we have come to expect from maps. These maps may even be especially disorienting in a world where expertise is often dismissed in the United States–not only by the U.S. President, but out of frustration at the inability to distance, diagnose, track or supervise the disease that is increasingly threatens to get the better hand. Have our visualizations been something of a losing battle, or a war of atrophy we will not win? Or do we even know what sorts of data to look at–indeed, what is information that can help us process a sense of what might be the geography of the contraction or the transmutability of the virus? Is the virus eluding our maps, as we try to make them? These sort of questions of making sense may be the process of science, but they trace, suddenly, a far steepder learning curve than we are used.
A dismissed biomedical researcher who ran efforts to develop a vaccine cautioned that we still lack that the failure a trusted, standard, and centralized plan for testing strategies must play a part in the coordinated plan “to take this nation through this response.” Dr. Bright, who was abruptly removed last month from his position as head of the Biomedical Advanced Research and Development Authority, bemoaned the limited statistics, alas, in large part as fear of providing too many tests–or fanning the flames of insecurity that testing might promote in the general public and in our financial markets, seem to have created the most dangerously deceptive scenario in which the United States seems to be committed to projecting confidence, even if it is the global epicenter of the pandemic.
Have we developed a language to orient ourselves to the scale of emergency in the spread of COVID-19? While we turn to images of natural disasters in describing the “epicenter” of the outbreak in Wuhan, this hardly conjures the species jump and under-the-radar communication of the virus that was not tracked for months before it emerged as a global threat. In tracking COVID-19 globally, or over a broad expanse of nations or states, we often ignored the pathways by which the novel coronavirus is spread in crowded spaces, where the single strand of RNA may hang in droplets that linger in the air, and are looking at the small scale maps to track a microscopic pathogen. But we are increasingly aware the spread of these strands, of the virus SARS-CoV-2, that infect populations along increasingly unequal fault lines that divide our cities, nations, health care systems, and crowding, or access to open space, are all poorly mapped in the choropleths into which we continue to smooth the datasets of infections and hospitalizations. While the problems are posed for national health services in each region, the devastation and danger of overloading public health systems and hospitals outweighs are local manifestations of a global crisis of the likes we have not confronted.
2. And the crowding of such numbers beyond the buffers that began with lead to a visual crowding by which we continue to be overwhelmed–and will have been overwhelmed for some time.
For although the global pandemic will clearly be with us for a long time, spatial narratives might be more likely to emerge in networks and in forms of vulnerability, in ways that might reveal a more pronounced set of narratives for how we can respond to a virus than the deep blues of even the limited and constrained datasets that we have, as we struggle against the blindness we have in containment and mitigation, and the frustration of the lack of anything like a vaccine. (This pandemic is almost a metastasis of the anti-vaxxers: confirmation that a vaccine cannot check a disease, it gives rise to concerns that vaccinations might have left us immunologically more vulnerable to its spread . . .and a sense that the hope of eradicating COVID-19 by the availability of a vaccination in four to five years will be widely resisted by anti-vaxxers and their acolytes, to whom the pandemic has given so much new steam. Yet as the virus interacts with the viral posting of anti-vaxxers resisting social distancing or collective policies of response, the stresses that exist in our society will only be amplified.) And if as late as February 24, only three laboratories in the United States did test for COVID-19–artificially lowering public numbers–even confirmed numbers through March and April were as a result tragically low. Could maps even help to track the disease without a testing apparatus in place?
The prestige of the data visualization has been a basis for reopening the nation. Yet if less than a tenth of the world’s population has yet to be exposed to the disease–and perhaps only 5% of the American population, in one estimate, if not lower–the virus is bound to be endemic to the global landscape for quite a considerable length of time. At the same time, one must wonder if the many fault lines that have created such peaks and valleys in the virus’ spread, if confirming its highly infectious nature, to be sure, are not removed from us in some degree by the smooth surfaces of the screens on which we watch and monitor, breath bated, with some terror, its spread, unsure of the accuracy or completeness of the data on which they are based but attentive to whatever they reveal. In many ways, these maps have created an even more precarious relation to the screen, and to the hopes that we find some sign of hope within their spread, or hope to grasp the ungraspable nature of COVID-19.
These datamaps suggest a purchase on a disease we don’t understand, and we don’t even have good numbers on contraction. Yet we are discussing “reopening” the United States, while we do not have anything approaching a vaccine, let alone the multiple vaccines that medical authorities desire before resuming social contact at pre-pandemic levels. How to process the data that we have, and how to view the maps not only by hovering, zooming in, or distancing the growing rates of infection, but tracking the virus in spaces, mapping levels of infection against adequacy of testing, mortalities against comorbidities, against with the chronic nature of the virus must be understood, as well as levels of hospitalization levels; and distinctions or mutations of the virus and against age ranges of afflicted–by, in other words, drilling beneath the datasets to make our maps’ smooth surfaces more legible, as horrifying as they are?
Can we use what we have to pose problems about the new nature of this contagion we don’t fully understand, but has been mapped in ways that seek to staunch fears of a decline in the stock market, as much as an emergency of public health, with up to one third of the population at risk of infection? The instinctive reaction of the Trump Health and Human Services to create public-private “community testing sites” for drive-thru or drive-up testing at Walgreens, CVS, Rite Aid, Kroger and other pharmacies seems reflexive for a government wanting to minimize federal overhead, but a far less exact means, and a far less intuitively sensible basis to attract potentially infected individuals to sites of public congregation. The hope of Verily–a subsidiary of Alphabet, whose Project Baseline boasts the slogan, “We’ve Mapped the World, Now Let’s Map Human Health,” in a bizarrely boosterish rhetoric, aggregates medical for medical screening in California–
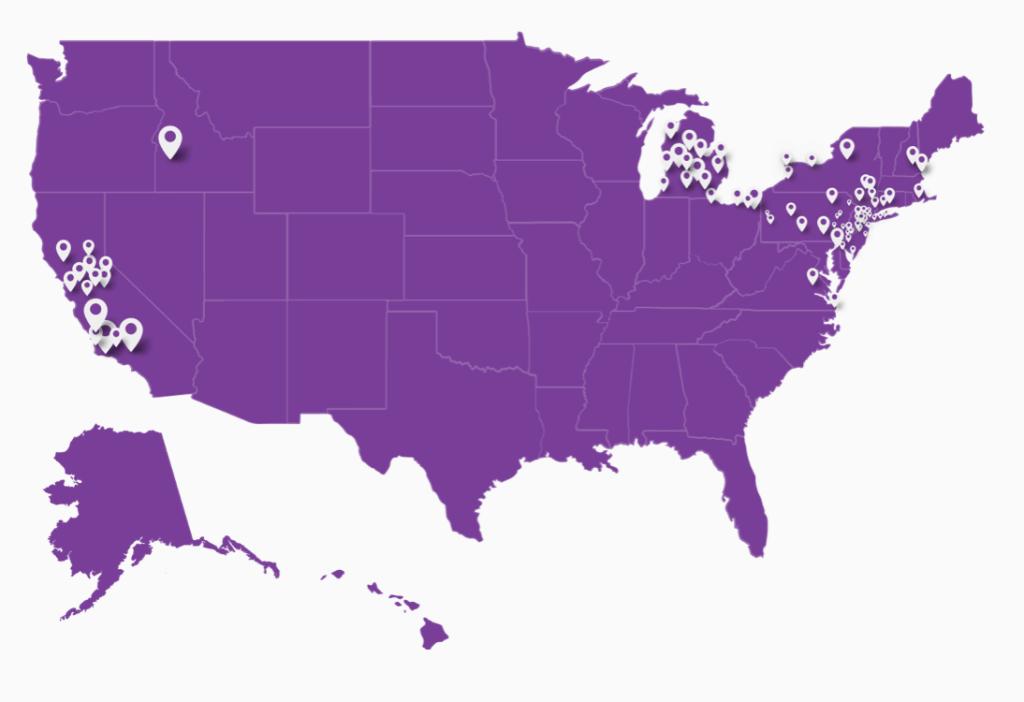
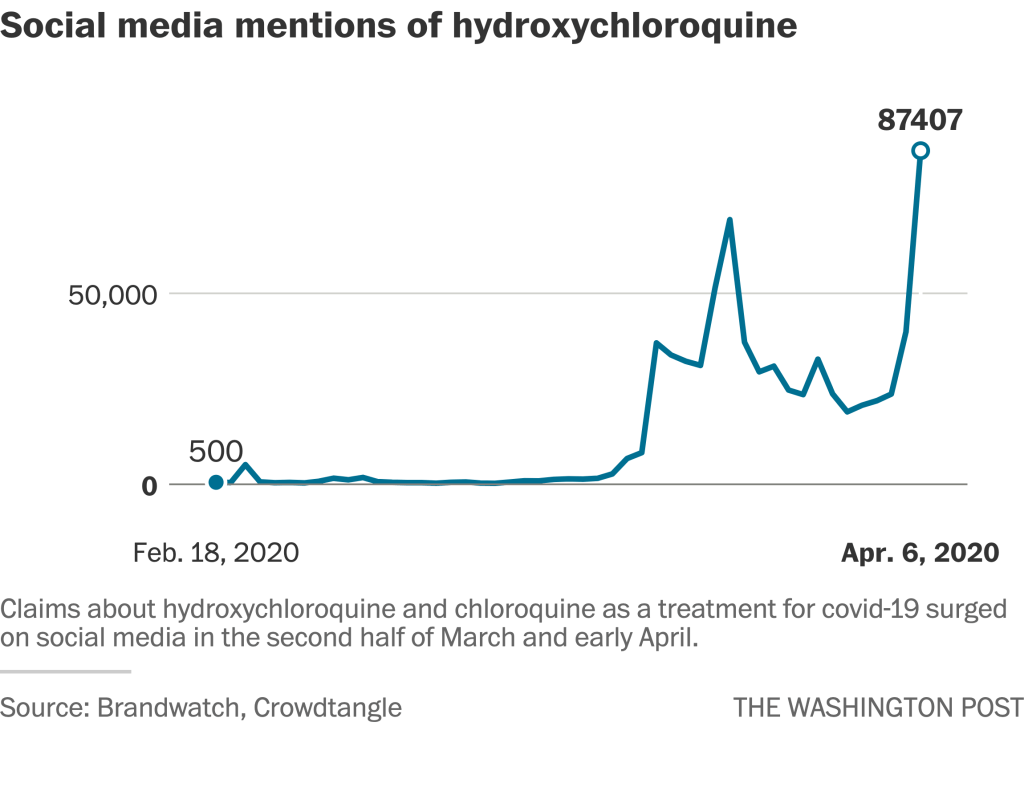
–and select states–was the primary response that Trump had promised of a network of drive-up testing sites that has never materialized, even as it expanded to a hundred sites in thirty states. After Walmart opened two sites, and Walmart 40, the difficult accuracy of creating multiple testing sites was prohibitive, the testing sites that were rolled out with the assistance of private entrepreneurs that Jared Kushner enlisted, that filled the absence of any coherent public health response–perhaps, terrifyingly, in concert with his brother’s health care company, Oscar, which also partnered with CVS and some of the same pharmaceutical services, focussing on drive-thru sites more than sustained medical care, focussing largely on calming retailers who feared the arrival of infected patients on their parking lots, more than on the efficacy of testing, which they didn’t understand. If only 40% of promised test kits were made available, the absence of providing staffers or selling, as in Massachusetts, self-testing kits–and failing to provide many in large cities like New Orleans, as if to keep the final tally of infected artificially low. Even if the Center for Disease Controls had never done clinical tests on hydrochloroquine, whose dangers on humans were not studied, and despite some benefits of the antiviral on cell cultures, none appeared in mice, the drug was promoted widely on social media as late as April, although its mention on Twitter grew, even as the government delayed any roll-out of testing sites.
The demand to calm the nation, a position dangerously close to concealment, delayed action on a wave of infection that President Trump had long sought to deny, claim to be overblown, or call Fake News. The lack of a public testing initiative, and rejection of the tests of other nations, forced the United States to adopt a disorganized go-it-aloneist approach, akin to isolationism, not benefiting from the potential ties to Chinese doctors’ response, or the testing kits that would have been available that the World Health Organization (WHO) had suspected since January, and made test kits for poorer countries that might be replicated in the United States–which chose to make its own tests to ensure the highest quality. When WHO had urged countries “test, test, test” for the coronavirus to contain its spread, the global health organization provided 1.5 million tests to 120 countries who lacked the ability to test by March 16; the United States went without the diagnostic tests developed in Berlin by la Charité, implemented in Germany. If the United States had submitted a test to WHO as well, the German test the health organization adopted was never used or ordered–and by mid-March processed a sixth the specimens as in Italy, with found over six times as many cases, and an eleventh as in South Korea, which found double the cases.
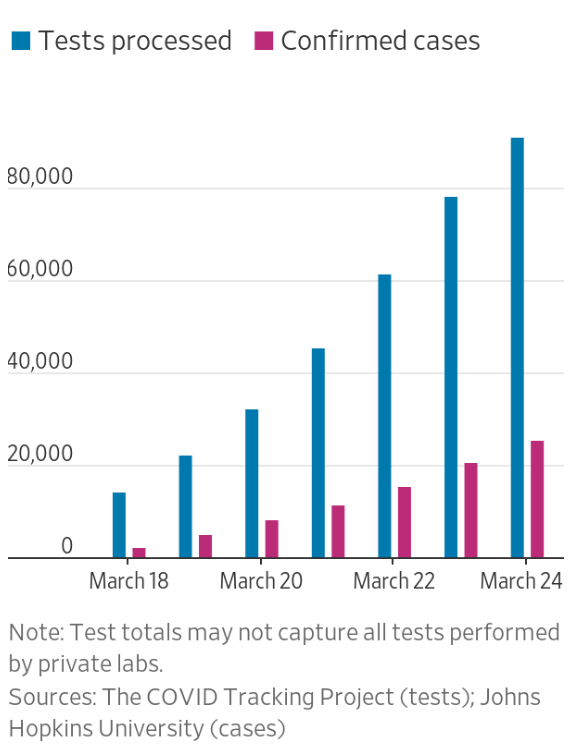
By April, the picture had improved, but not much.
And based on later data of the virus that spread to other American cities, the virus that had infected so many in New York seems to have spread to other American metropoles by May, as we were still awaiting broad testing.
After false promises of providing eight million accurate coronavirus tests to Americans by mid-May, the FDC seems to have decide to rely on the distribution of test kits that relied on automated testing of Thermo Fisher. The private company that provided them still lacked clear oversight, and the machine was unknown to Medicare’s innovation chief, and based on trust–but its adoption reveals a broad break in public trust of the public administration of tests for COVID-19 infections, even as death tolls mounted across the nation, focussed in New York, and would rise beyond the fatalities of Americans in all twentieth century wars. It demands to be seen how much the failure to provide testing, in the face of a massive waves of death that ran through cities, were not a basis for the disruption of a social compact within American cities, that prepared them for the summer of 2020.

The network expanded to those places judged to be of “greatest vulnerability,” but leaving multiple underserved communities at considerable cost to developing an accurate databank. The initial decision to ration test kits played out by early May into a situation when only 3% of Americans were tested, dangerous for a virus who displayed few signs of the illness when most contagious. The fear of spooking the markets may have outweighed the need for responding to the health threat, suggesting the prudent nature of a reaction that would have most appealed to Trump to not rankle the public or provoke widespread panic, more sensitive to his public perceptions than the demand of his office..
The slow spread of the idea of “testing sites” in such public-private drives, as much as serve patients, created an absent baseline for public testing, to be provided by Verily’s Baseline platform not in a form of medical coverage or in HIPPA security standards, if it supports compliance. The project is intended as a roll-out of a new form of medical record keeping for the long term, not specific to COVID-19, or a minimal data collection service for initial run-through of a model to allow medical tracking and widespread screening and testing to compile public health data–not a means of ascertaining levels of infection, which prevented Americans from developing anything like a clear picture of the spread of the epidemic–even as we looked to the world, viewing the spread of the novel coronavirus through buckets and lenses of national sovereignty. Initial tests were confined to those who were within six feet of something infected with COVID-19 or had been in China or Wuhan. Unlike the regular updates on H1N1, SARS, or Ebola, the public health threat was minimized, and no clear infrastructure of pandemic response was created.
“Above all,” said Anthony Scaramucci about his experience in the Trump administration, “you must never make him feel ignorant.” Did an absence of medical expertise in confronting the disease Trump was able to field make it difficult to read the disease but as a possible threat to the booming stock market Trump viewed as his greatest accomplishment? The content at the metric of economic growth outweighed the absence of a cabinet-level position of public health. The problem of embodying the disease extends to how well we are able to bring ourselves to read the dizzying tallies of the infection rates we seek no longer to contain–there are no clear edges with the pandemic, almost by nature–and it may make far more sense to learn to map susceptibilities and vulnerabilities to the disease by digging into the large aggregates of infections that dizzy, but demand to be better grasped if they can be translated into health care, rather than alarm. And the deeper problem, that will be the focus of the bulk of the post, is the difficulties of scale at which we continue to parse the disease by localities, acting as if the geotracking that we developed for humans make sense to track migration of a zoonotic virus that does not know frontiers, but travels in pathways of shared space and surfaces, in ways we have not learned how to track.

And if we are constrained in mapping or processing COVID-19 by the resistance to consider it a global pandemic, retaining national counts as we depend on national senses of order, well-being, and national health services if not universal health care, the alleged national problems of confronting COVID-19 should not conceal the the unfolding narrative is global, and global in ways we are not used to map–especially not in our narratives of pathogens’ transmission, or in distracting narratives of national levels of infected populations in different nations–as if the virus respected boundaries, or tabulation practices were uniform or uniformly distributed across the globe. The limited data we have for our maps, and frustrating inability to frame narratives from the maps, reveals the dependence of good data visualizations on good data, and the complexity of trying to map the virus on sufficient scales to comprehend its global spread. Perhaps this is because there is no clear narrative that has emerged, but it is also because we are viewing the sheer numbers of reported infections in a freeze-frame, overwhelmed by needs of mitigating its spread, no longer able to contain the virus that we seem destined to live with for a far longer period of time than we were able to admit.
And the Distractor-in-Chief seems bound to introduce red herrings that obscure the spread of COVID-19, imagining that not wearing a mask is a sign of strength and resistance, as he questions the accuracy of testings, rather than using Presidential authority to expand testing nation wide in a true emergency–the first encountered, perhaps, in his presidency–although abilities of mitigation are not being considered broadly so much as deregulation, tax breaks, financial incentives, and while best practices have not been defined. As if embracing the false data maps of national differences in tallies of infection for his own ends, Trump has insistently warped the need for international global virus response to national competition for lower numbers, pointed the blame abroad, and failed to expand testing in critical ways, as if to obscure the map intentionally and muddy our waters. (Indeed, without needed testing, we don’t even have a sense of the accuracy of the maps we make.)

As we move toward hopes for mitigation of the virus that has explosively arrived in our major cities, penitentiaries, centers of butchery, old age homes, and hospitals, we face problems of lacking a close-grained maps able to track the different scales by which it has been contracted to gain much stability on the virus’ spread that might give us a better bearing on its future, but are seized by often unwarranted senses of false security from existing maps. While infections spread around the globe, it was somehow fitting that the American President spread disinformation, seeking to provide encouraging spin, probably with the advice of Jared Kushner, a man who believes spin is all, as his father-in-law, as Laura Ingraham and other Trump surrogates declare hydroxychloroquine’s availability to be the “the beginning of the end of the pandemic” as we know it, as infections confirmed in the United States approach 900,000.. For the logic of the “America First” premise on which Trump was elected President, and is conducting a new campaign for re-election, run against the very global nature of the pandemic.
3. While the pandemic is a stress test for our societies, and for the global response to a disease that has spread along the very lines that bind the world together–from airline routes to public transit, from markets and public spaces to institutions of learning, public health, schools–it is also a stress-test on mapping tools, putting new pressures on how we can better track the diseases, reveal the continued validity of maps and tracking apps, and use sufficiently finely grained tools whose dashboard remains global by default from March 11, when it was declared a pandemic,–reflecting global spread of confirmed infections across seven continents–
–to early May, when the United States, after having subtracted itself from global health authorities, and cut its substantial contribution to the World Health Organization, which it accused of undercutting American interests, had itself become the new “epicenter” of infections worldwide.

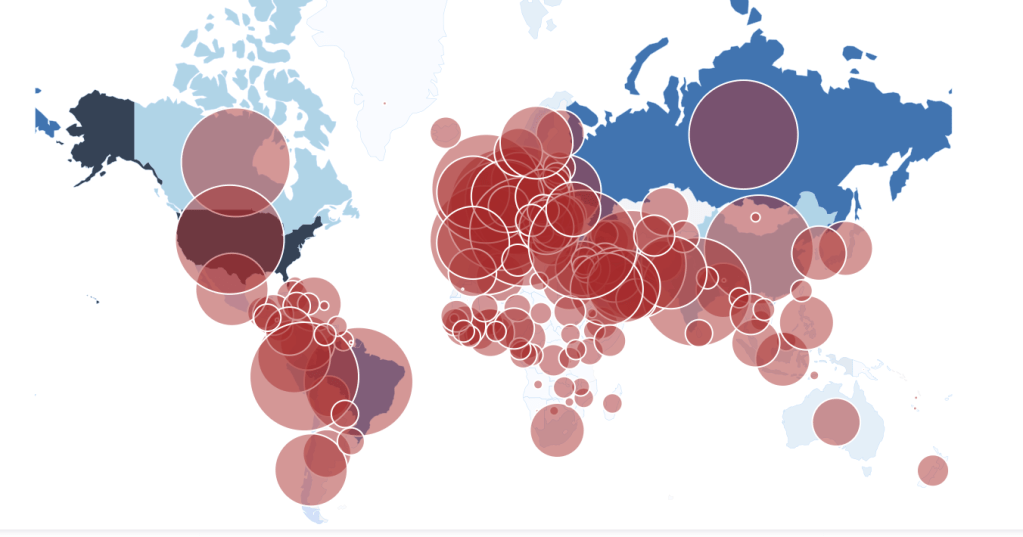
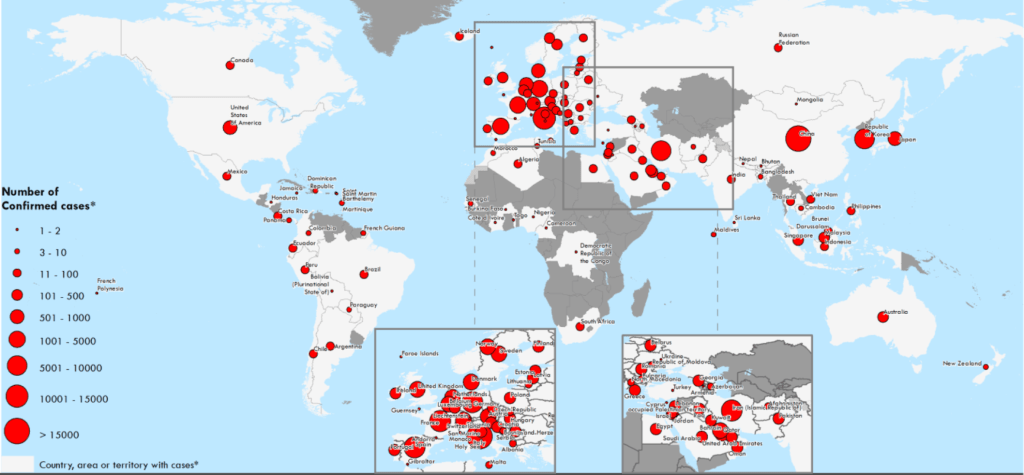
The maps are striking, but the small-scale conventions of their global purview are almost designed to mislead. These aggregations of confirmed cases of the disease, that show a global map riddled with red dots, fail to describe the pathways that the virus takes, although they stand as a riveting proxy for its spread across a national map. Toward the end of March, the global nature of the disease was overwhelming, identification of “hot-spots” overwhelming, and tallies of cases and mortality cognitively overwhelmed. Was this globalism, or globalization as we had never so vividly seen it, presented on our screens in vivid color, a newly frozen world trying to process its losses and their scale, as we finally acknowledged the global pandemic? Could we re-orient ourselves to the global scale of the pathogen’s spread?
Or did we need a new sense of the multiple scales on which COVID-19 was transmitted by human contact in crowded spaces the increasingly overlap with one another–and another of the United States’ increased separation from the global accords before the disease? If lingering diseases were associated with poorer countries and environments, the global migration of the novel coronavirus has become a point of fascination and a terrifying passively received spectacle on global media, transcending any government’s control, and reminding us of the difficulty of containing the ease with which it is contracted, drowning the viewer in confirmed cases with little actual geographic or demographic specificity and little distance.

We faced an immediate existential level of meaning and alarm in the appearance of infections that seem to proliferate like an actual organism over a huge expanse, triggering a sense that there is not only no “escape” from the virus, but that is proximate to much of the world’s population. And if the Trump administration has almost worked to prepare us for a global pandemic in the cruelest of ways, by cutting back our own scientific presence in the health care system in China to monitor emergent zoonotic pathogens like the novel coronavirus SARS-CoV-2, or the international branches of the CDC and NSF, or even by demeaning the recommendations that the CDC and other health officers offer the nation as overly restrictive, the failure to prioritize or value testing and best practices of the mitigation and containment of infection, which began far earlier than the United States officials or government publicly noted.
We watch the progress of the pandemic on screens, while sheltering in place, uncertain of how what is moving across the country can be tracked with precision. The drama of mortality scenes that have multiplied to become far more present in our consciousness than we ever thought possible in a modern era seem to haunt us, destabilizing our sense of life and death, leading us to turn to cultural resources we hope will provide some form of orientation, because the data is so hard to look at, and so difficult to parse. Never has Washington, D.C. seemed more removed from a global crisis, and America, the new epicenter of the virus’ spread, seemed harder to orient ourselves to as we enter a new stage of emergency and a new status quo of disorientation, the inequities of health care and paucity of testing equipment parallel a problem of gaining bearings by our maps.
The pandemic outbreak was for far too long mis-mapped as lying only in China–exploiting the rhetoric of nationalism not commensurable with the meaning of a pandemic–before the narrative became global, if it of course we long suspected that it was not only local. On January 30, Commerce Secretary Wilbur Ross affirmed energetically to the nation the infection afflicting up to 8,100 in China “will accelerate” jobs’ return to the US, predicting a “reshoring to the US. and some restoring to Mexico” that used the obsolete markers of shores as a unit of economic integrity that should have left us worried for its dissonance with an globalized world, as interruption of supply chains affected American industry based in Hubei, from processors to electronics: but as Apple hurriedly shifted jobs from computers and phones from China, Trump’s desire the United States companies act to relocate operations from China seemed more in sight as the coronavirus was almost readily interpreted as, in fact, a financial bonanza for the United States.
Is it surprising that there is not a health officer in the Cabinet?
The dominant White House interpretation of data about the disease is a logic of the continued extraction of profits, not only of tax breaks and stimulus packages, but outright profitability from pharmaceuticals that have no clear relation to the virus (hydroxychloroquine . . . ); tests that prove to offer little useful accuracy in testing (the “great test” Trump promoted from Abbott Labs, ID NOW . . . ); limits of the reliability of serological tests; and the involvement of members of the “first family” in automated health advice that provides a poor, tragic, empty substitute for health care. Trump had promoted hydroxychloroquine on March 19 as a “game-changer,” echoing the words by which FOX’s Laura Ingraham endorsed the drug in an interview tie Gregory Rigano, a Long Island attorney who had been promoting the treatment in a much-retweeted GoogleDoc, broadcast March 16: the broadside designed with the appearance of scientific validity incorporated the theories of French virologist Didier Raoult–whose work had spurred a rise in internet rumors as to its efficacy, from late February to early March: Raoult’s findings gained currency through block-chain investors and Elon Musk, who valued the lack of clinical validation or trials, claiming hydroxychloroquine “efficient on SARS-CoV-2, and reported to be efficient in Chinese COV-19 patients.”
Trump promoted the drug championed by investors and speculators without clinical grounds: without endorsement from the medical community, the rash of social media interest led to accelerated stockpiling and strong-arming scientists to approve an emergency authorization of the antimalarial for widespread patients hospitalized with COVID-19 infections. With revaluation of real dangers of cardiac arrest after taking the anti-malirial was it withdrawn, and the National Institute of Health undertaken the large study of the very untested cocktail of drugs Dr Raoult had promised, after stockpiling of twenty-min million hydroxochloroquine pill Despite fears of its ties to paranoia and psychosis, and cardiac arrest, Trump endorsed the dangerous drug in a widely shared March 21 tweet, following discussion Dr Raoult, who found the President a true entrepreneurial mindset needed to promote a drug without testing: the drug during White House briefings in early April, and advocating its use by non-symptomatic Americans take the drug–before telling the nation he was regularly taking it himself by mid-May. At that point, the FDA withdrew its qualifying cautions of side-effects, as Trump gloated that “What has been determined is [the compound of drugs] doesn’t harm you,” attacking studies that questioned its safety as partisan. While the Food and Drug Administration restricted hydroxychloroquine as a coronavirus treatment in hopsital settings, given “reports of serious heart rhythm problems” in virus patients who had received the drug, Trump questioned the study as “a Trump enemy statement,” deploying Manichean logic of a paranoid by discrediting the Veterans Association study as the work of “people who aren’t big Trump fans,” elevating demonization above scientific verification and linking the drug to his brand. Was the popularity of the drug to boost collective consent to his opinions amidst a public health emergency as COVID-19 infections grew across multiple states.


Was the promotion of this potentially deadly drug that has not been tested an attempt to restore trust in an administration that has failed to assemble a coherent public health strategy, but eager to promote a market for drugs ? The weaknesses reveal the dangers of trusting in “the private sector” Trump celebrated to respond to a public health crisis.
After the fourth product form Abbott Labs testing for COVID-19 was fast-tracked for “emergency use authorization,” an emergency authorization of hydroxycholoquine issued, and 30 million tests ordered for May with 60 million to be shipped in June, for administration at CVS stores for drive-through testing in mid-April, were serious questions raised about the very tests intended to replace WHO test-kits the United States had refused. Whereas Trump had promised that the fast-tracked would start “a whole new ballgame” in containing COVID-19, it seems as if it may be the same game of for-profit corruption: with the efficacy questioned as of clinical viability by Langone Medical Center, the test is tied to a health insurance company Kushner and his brother Joshua founded, Oscar, whose fast-tracking eliminating review strikingly occurred after the FDA tightened rules for coronavirus antibody tests, based on Abbott Labs’ own claims.
Trump seemed to be defending American enterprise in providing tests in his public addresses. What seemed product placement to many–if not an endorsement–may have backfired as an attempt to seem in possession of actual testing technology. Rather than accompanied less by an effective roll-out overseeing state testing, the promise to provide a list of labs promising to fill tests that has not produced viable results for state health agencies, and insecurity about the clinical value of testing devices’ results, prematurely proclaiming his administration’s victory over the pandemic.

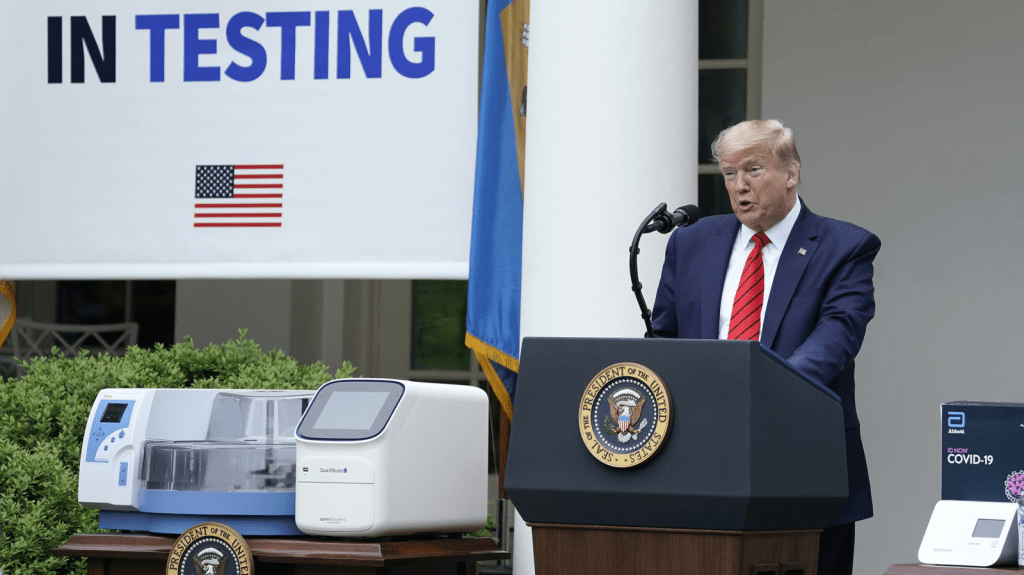

Seeming every more like a TV host, or as if he were foregrounding a prize in a series of Reality TV, the President-with-Teleprompter promised a revolution of diagnostic practice as if it ws about to arrive, yet again, even though the promise of further testing and better data did not arrive.
Was this even recognized as a crisis in public health? Far from it, for this administration. President Trump’s own economic advisors looked at maps with little interpretive skill or outright duplicity, noting “We see no material impact on the economy,” leading Larry Kudlow to insist “the pandemic is, of course, in China, not the United States,” underlining “no material impact” on America’s vibrant economy.

Was this a misunderstanding, distortion, or pathological? Was not any pandemic a global event? Americans would only rush to clarify the meaning of “pandemic” a week into March–even as some within the administration noted the absence of any protection for the novel coronavirus in terms of a cure or vaccine left the country vulnerable, as if it was failed to be included in the pandemic or could be localized. In early February, the government was assuring the nation that the United States has only had 13 confirmed cases of the virus, on Feb. 11,–mis-mapping the virus to dissuade closer scrutiny of the pandemic’s scope–“pandemic” only really jumped as a Google search after March 9 in the United States, despite a bump in searching in late February: we were watching something else on our screens, bracketing the possibility of a pandemic. Yet even as we acknowledge the pandemic, the flatness of the maps we watch on screens seems all to easy to place at a remove, and paralyze us before its spread, much as they mask the divides within the nation that is exposed to infection or the topography of risks that might be managed or addressed.
The rhetoric of COVID-19 was tantamount to an epidemiological re-centering, mis-mapping of attention in a time of emergency. The adoption of the talking points social media supplied through the that was born in the anesthetized cocoon of social media offered a meme more than a logic: the retweeting of the charge that linked China, the danger of the novel coronavirus, and the Border Wall conceit was born in the feed of a combative coordinator of right-wing student outreach, eager to map the danger Trump promoted in combative terms: the meme tying protection a “Border Wall” could offer against infection only amplified Trump’s earlier assertions it was the border wall that would prevent the entrance of the coronavirus COVID-19 on late February, in Charleston, S.C., turning attention to his signature piece of policy, so often described as “going up fast” and recasting it as a basis to stop the spread of coronavirus, which led Trump to retweet the specious speculation of a man who cut his teeth on Breitbart: “With China Virus spreading across the globe, the U.S. stands a chance if we can control our borders”–to his 77 million followers. The mismapping gained so much traction to identify the origin of the novel coronavirus that the geographic origin was elided with national agency in talking points of Trump’s followers, as the virus–blamed on America in Iran–was blamed on bad human actors for having globally circulated or mismanaged without credibility:

The March 10 tweet was expanded in Trump’s address to the nation that described his closure of borders as a response to the COVID-19 outbreak, as if a proven panacea among States of Emergency might credibly recycle the maps of previous one.s that he had welcomed on the southwestern border Even as Trump endorsed mapping of a containment of COVID-19 in Europe and China, he seemed to manufacture a sense of national safety removed from the actuality of global viral transmission, whose rates of infections were already exponentially growing in the United States.


It is amazing that his response is to close the borders. Has to be something weirder than denial, as you suggest. Border closing as both cause and “cure”.
The denial seems cognitive, but inability to acknowledge the responsibility of governments suggests a stunning lack of prioritizing public health safety. The script of demonizing foreign countries was on auto loop, and the world will suffer!