
16. Cartographers are increasingly aware of the dangers that the color choices in a map can work to “strike fear when it is unnecessary” in their viewers, but what is the value of this mapping precept when most of the nation is paralyzed by fear? The problem we are all wanting to extract from these maps are not only what the routes of transmission of the disease are–we are terrifyingly paralyzed by the routes of transmission and fears of contracting the virus, turning to hand sanitizer, hand-washing, masks of any sort, and perhaps unnecessary clothes-washing, and then to making home-brewed hand sanitizer, but the expansive toll it the hardy and so far unmutated single strand of RNA SARS-CoV-2 is moving among Americans across space–and where we stand in relation to this progression of infections that we have no idea of how to treat.
But they would also be more empowering, more able to describe the transit and possibility of containing the disease as it travelled in space, and might promise to better orient ourselves to its spread.

As if haunted by the cumulative weight of death, and astonished by the exponential spread of the disease, we tracked COVID-19 misleadingly, if appropriately to its cognitive weight, in cumulative fatality counts, Dr. Joel Salinkio observed in mid-February, as if attempting to comprehend the scale of mortality rates of apocalyptic scale. The sense of a war against an unseen and invisible microbial enemy no doubt reconfigured the world outside of the borders, as we have been enjoined to understand the world in America. But we did a disservice in looking at the spread of the disease from Wuhan within the box of a nation–which makes sense here, because we are looking at data from one national standard–as if to contain its miasma, but there is an odd dissonance between the space-age monitor of a global map and an almost miasmatic image of disease that is more akin to medieval medicine removed from both course of the infection or its progress in individual bodies where it lives.

But if some describe quarantines and “Shelter-at-Home” directives in states as “going medieval,” it is more likely that the difficulty of underestimating the persistence, dangers at which health care workers put themselves in dealing with COVID-19 patients, and the persistence of pathogens in the air and the long range of pathogenic payloads in relation to those who suffer from the virus expose far more health care workers than familiar from modern clinical settings, and under appreciate the duration, distance, timescale, and persistence of pathogenic payload travel, and health care workers’ potential exposure. We are almost, scarily, almost medieval in our lack of clarity about the infectious nature of the virus unfamiliar to human bodies.
There is no sense we can watch this unfolding of cumulative deaths of the sort that medieval viewers may have been more familiar as an “art of dying” to come to terms with a sense of near-certain onslaught of disease. But we might do well to configure the eventuality of the virus’ spatial spread outside the apparently miasmatic nature of the spread of infection shown in early “heat-maps” of the raging of the virus across China in mid-February,–as a misleading dashboard to navigate the virus’ global spread.
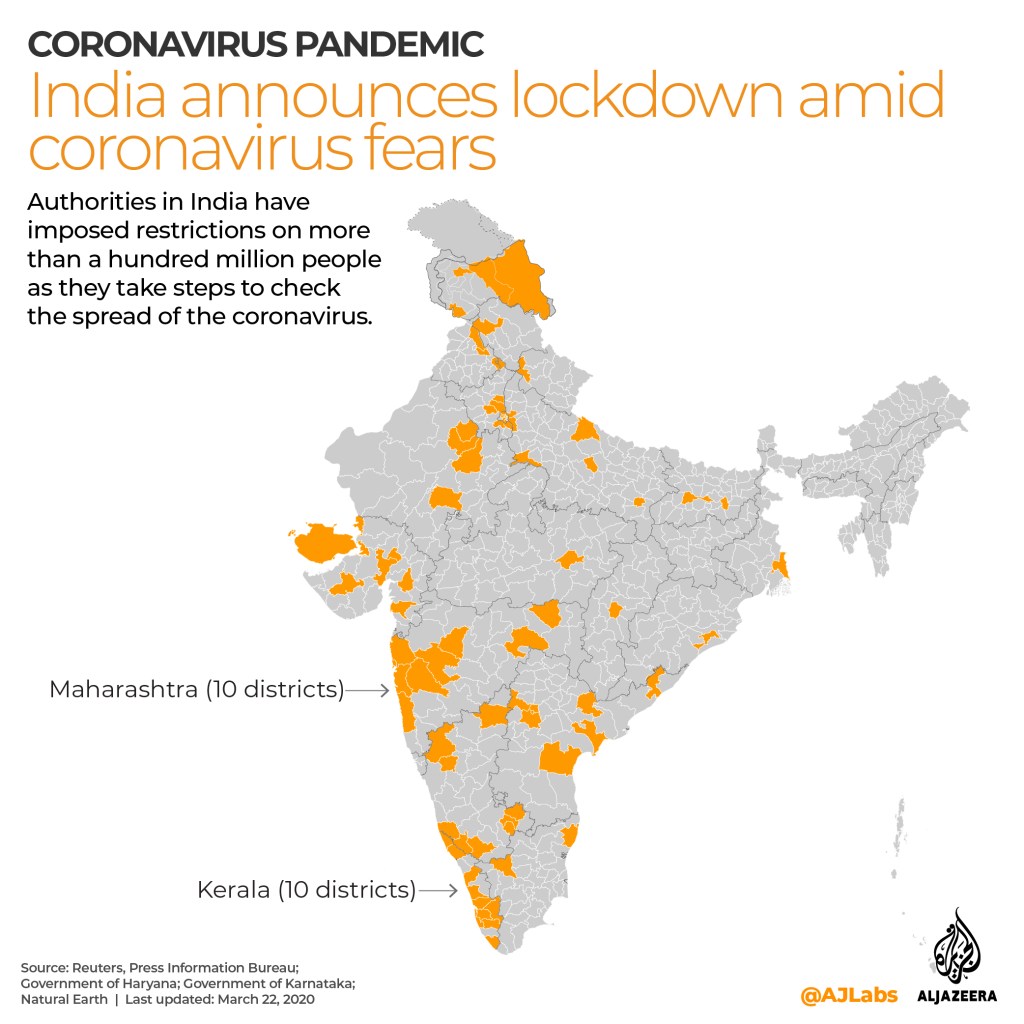
The sharps danger of retaining such remove from global currents is embodied in the ease with which Donald Trump’s government is removing the United States from its funding of the World Health Organization, removing the annual $400 million contribution at a time of need–and playing a lesser role in the planning of WHO intervenors. At a time of increased testing as COVID-19 as confirmed cases crest above two million. India, without funds or ability to test all its 1.3 billion people, is increasing surveillance by sending thousands of public-health workers to villages and towns to trace, track, and quarantine any contact with infected people, to isolate those infected as South Korea did with more testing kits, creating containment zones and isolation units for all testing positive. There are huge attempts to institute a “lockdown” on over a hundred million people, as Indian authorities have imposed to check the virus’ spread stand to expand a surveillance state with minimal resistance.
The lockdowns may only reveal how far apart many have come from the actuality of globalization and the reality of our interconnectedness. There was recently reported a stunningly clear sense the United States government indulged, in balancing alternate world systems views as late as January, as the virus spread globally but the few verified cases made it appear isolated in America in a few cases, even if its human-to-human transmission was confirmed. The attachment to place, in a weird way, trumped epidemiological reality; a stiff refusal of globalism obscured the pathways that the virus would take after the first man infected with COVID-19 returned to Washington from China, from Wuhan, on January 20, 2020, and another arrive in Orange County the next day, introducing SARS-CoV-2 to the United States.


It is amazing that his response is to close the borders. Has to be something weirder than denial, as you suggest. Border closing as both cause and “cure”.
The denial seems cognitive, but inability to acknowledge the responsibility of governments suggests a stunning lack of prioritizing public health safety. The script of demonizing foreign countries was on auto loop, and the world will suffer!