On a morning walk, my mind turning to Dr. Anthony Fauci’s injunction to exercise, I daily move between the many signs posted outside houses in my neighborhood congratulating graduates of the Berkeley CA public high school my daughter attends or Oakland’s School of the Arts and Tech, ending among million dollar homes sporting yard signs congratulating graduates of elite private schools. This is America, and not uncommon. The path I take traces yawning shifting divides of public schooling across America in the most blasé of ways. The uneven distribution of different schools barely conceals the deep divisions between schools and families seems to widen in terrifying ways as the coronavirus pandemic continues to ravage the nation. While we are shocked to learn that Donald Trump delayed informing the nation about coronavirus not to panicked markets, the lack of school policies stood only to magnify existing fracture lines: for the failure to provide any overarching vision left school districts with the football as decision makers they are unequipped to assess of learning requirements in remote settings of learning, and to bear the weight of difficulties in shaping remote learning programs without training.
Ill-equipped boards are asked to struggle in high pressure situations with finding ways of engaging students increasingly removed from one another or instructional settings. Increasingly, states are offering regional guidelines, but the absence of a national policy may rupture public trust with the very schools on which the nation most depends, now treated as swimming in a laissez-faire sea without guidesposts in an already disrupted educational setting, raising questions of graduations, requirements, baselines of school performance, or even study habits and the value of coursework and requirements for diplomas or graduation, as the educational market long an unqualified good in America stands to erode.
But if this might have been an opportunity for collective response, we have no evidence of any preparation to supplement what school networks offer, as if those who can afford the private tutors, off-site education, and private educational services are alone provided with continuing education, as other scramble to make up the gaps school closures create. Unprepared with a broader educational strategy in the midsized of a global pandemic, we have all in essence “left the library” of schools, pausing education or switching the nation onto a disembodied experience, that makes the old physical globes of schoolroom study seem emblems of a far less complicated past, when global topographies lay undisturbed beside books in cozy nooks, waiting, as it were, for new fingers to turn it with curiosity, while more and more schools are compelled to remain on the remote learning platforms to which they gradually shifted en masse over the month of March, 2020.


The status of education–and of school closures and now school reopening–became a sort of political football. Despite the readiness of a switch to remote learning and online platforms of education, school closures echoed a cartography of abandonment, in unforgivable ways: if closures were born of necessity, and disorientation before the pandemic’s spread. And the levels of insecurity that have been fostered in the desire for mitigation may remind us that the problem of COVID-19 has been a crisis of public education, as much as a lack of frontline workers’ protective equipment–PPE–or adequate testing.
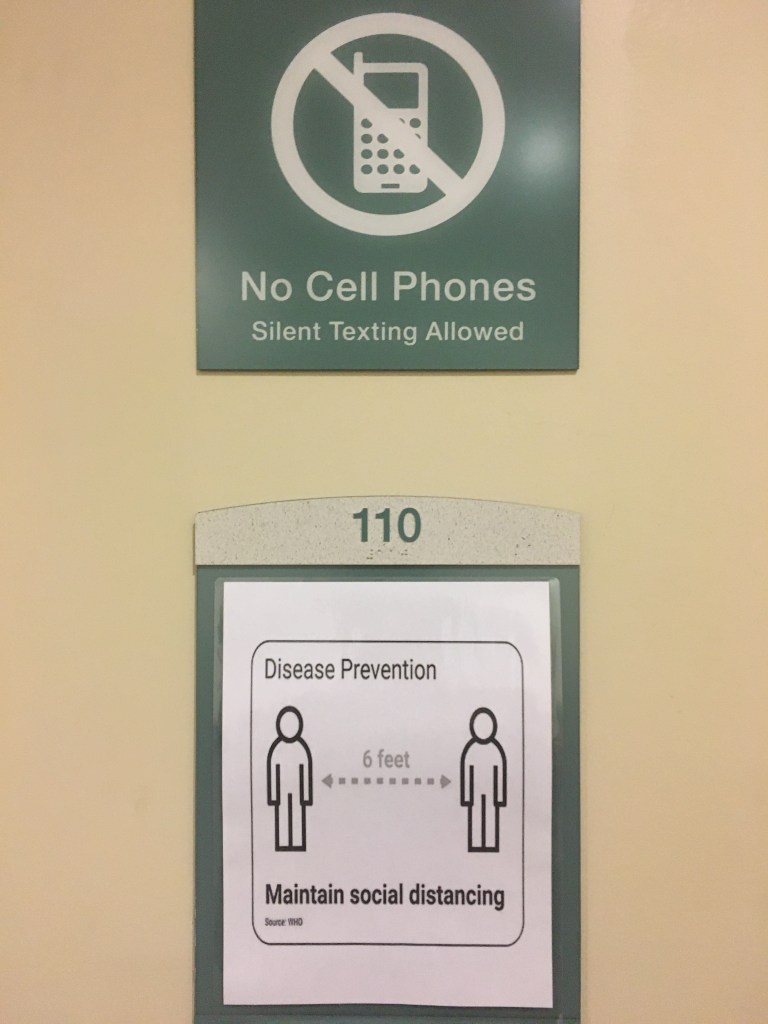
To be sure, the many functions that schools now provide across the social spectrum of the United States–meeting nutritive needs; offering social and emotional support and providing models outside the family for structuring time; minimal levels of health services–go far beyond being quantified by educational standards: by a magic trick of tests and quantification, government may have reduced education to metrics that erased their value as sites of community from the Bush administration, and led them to be sacrificed with deeper costs than many have registered. Without metric to tally schools’ dividends to students and communities, we omit the crucial educational role of instructing about coronavirus comportments–from regular hand washing to social distancing to mask-wearing, to bridge some of the enduring divides that have endured in the nation, with coastal “elites” donning masks more than the “heartland” of an expansive non-urbanized midwest.
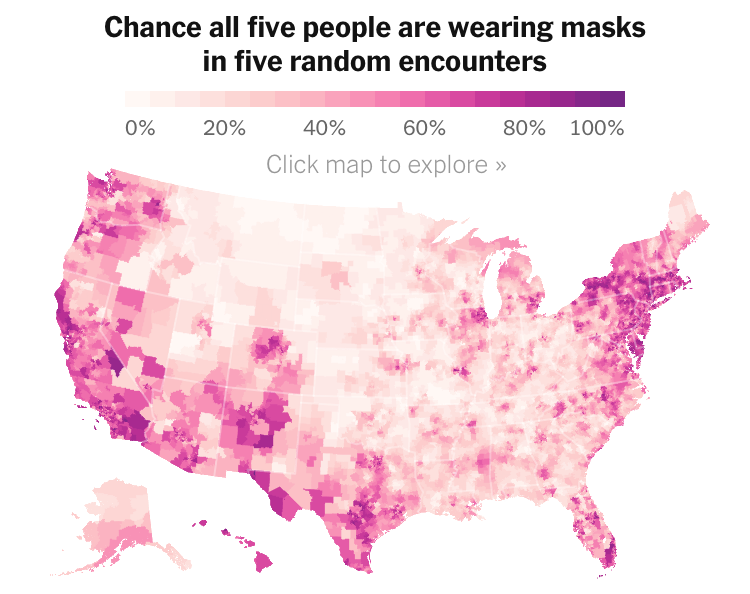
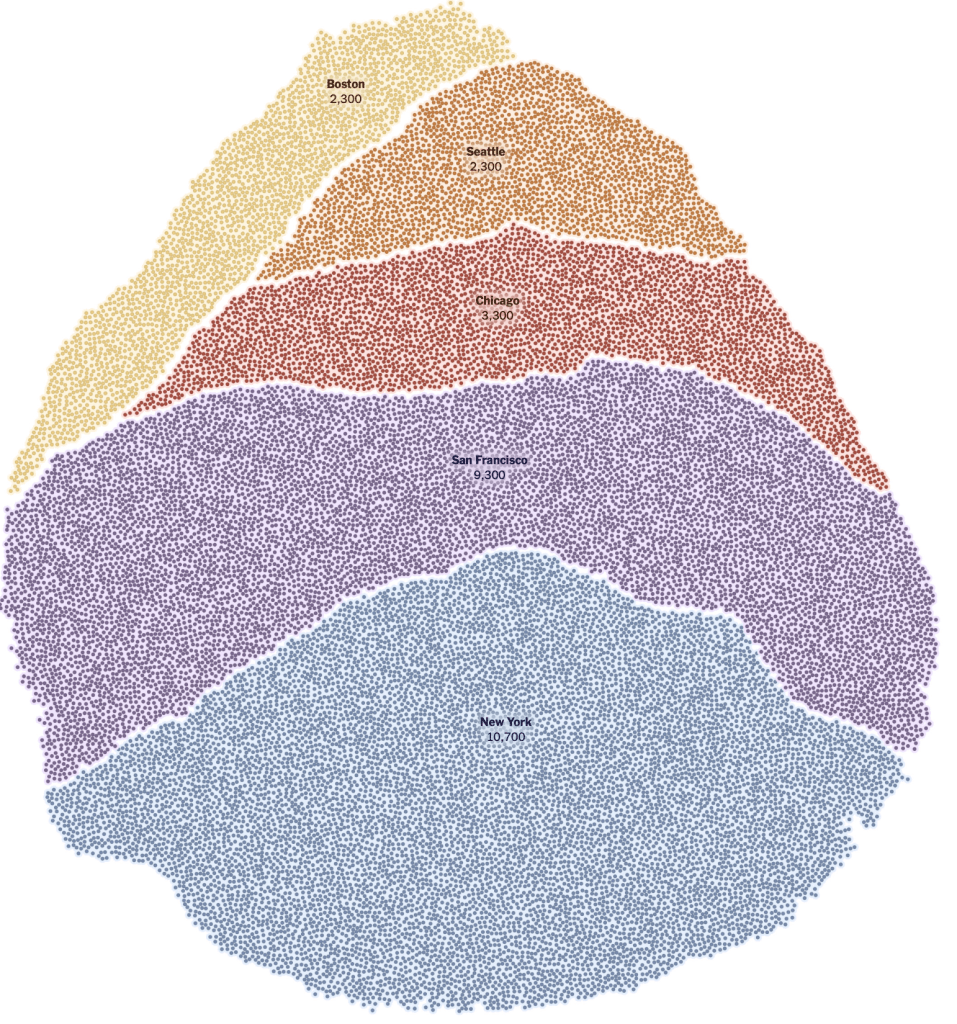
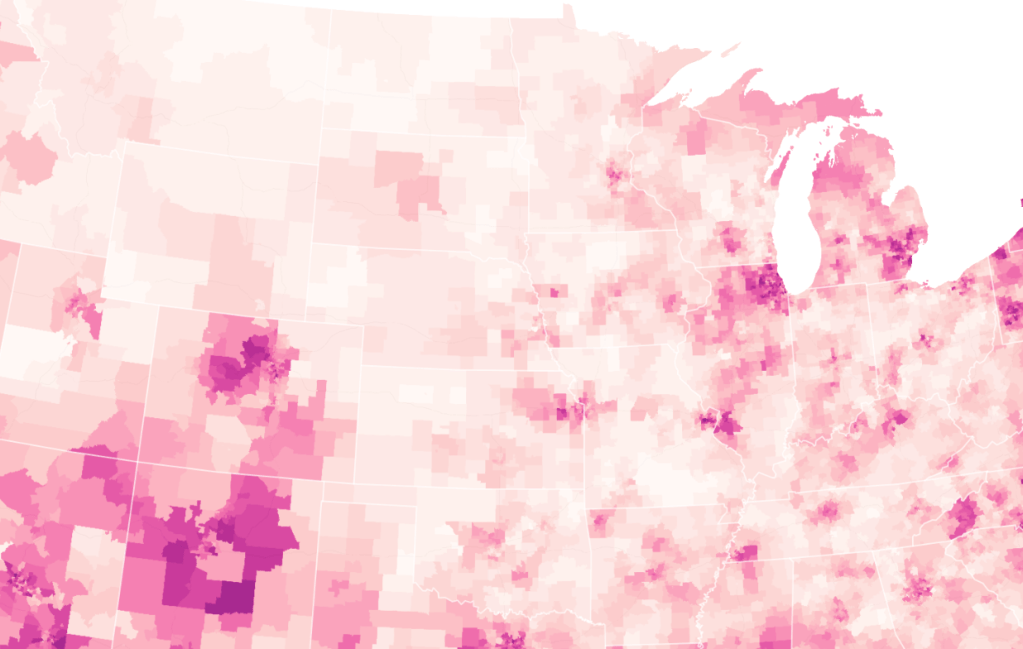
Is not the deep and tragic failure to not “educate” the nation to mask-wearing, sustained since the first cases of the coronavirus reached our shores, suggested the only the initial hot-spots where infections ravaged communities in the New York tristate area, Seattle, the Imperial Valley and coastal California, and central Texas are sites of mask-wearing, with Chicago, Detroit, Denver, the southwestern border and coastal southern Florida and Tallahassee. Only a fifth of the time or less were all five people who might meet at a large part of the nation likely to be wearing protective masks.
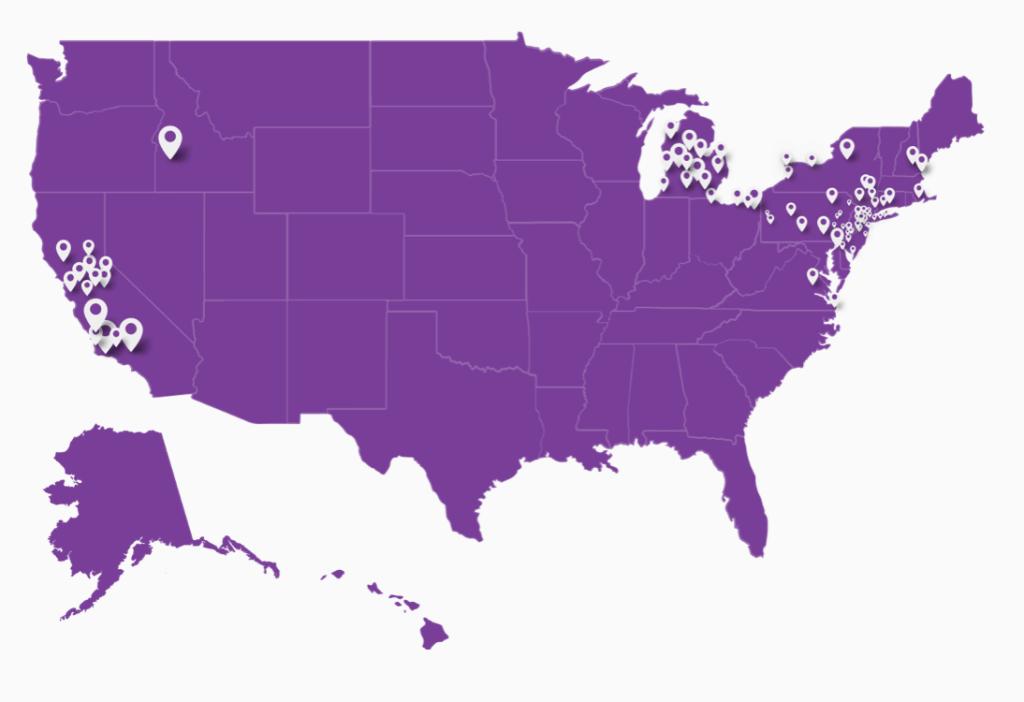
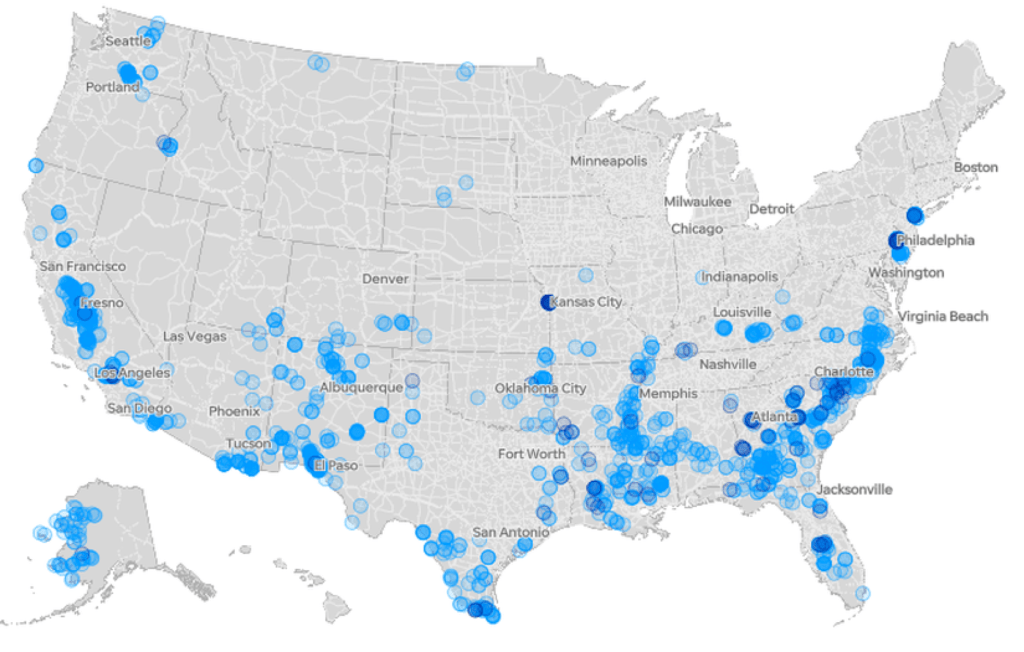
Why is such a paucity of mask-wearing continuing save an absence of public health education? There is a predictable if terrifying congruence with areas that were themselves, by the proxy of underserved medical communities Mitchell Thornson mapped, also by a Mapbox distribution of commute-based health centers, rather than by counties, to suggest the sites most vulnerable to disasters such as viral infections: even if the promise of a complete count of infections recedes, the inhabitants of some 300 counties underserved by federal health services suggests fault lines of future sites of vulnerability, that may accentuate with continued school closures.
These steep inequalities of health care suggested a very broad difference in those able to weather and sustain COVID-19, to which the Trump administration seemed blind. School closures created insecurities for American families was perhaps not different from globally, but they lacked any support network: social support had withdrawn to schools in the United States more than other nations. The lack of any narrative of the sudden closures, and interruption of human contact and resources that followed, were deeply disorienting. And the lack of oversight from a government that one expected, perhaps with little grounds, to provide a sense of purpose and oversight in an unprecedented health crisis was, unbelievably, punted to the states, and from the states to local school boards, utterly unprepared to cope or plan–as admittedly, even are many medical specialists and health professionals–with the scale of a pandemic.
It seemed like a charade of government effectiveness; Secretary DeVos shifted from leniency, lack of coordination, to steadfastness concealing unprecedented circumstances. And the recent possibility that private schools and sites of instruction will be allowed to open their doors, while poorly funded public schools serving adjoining communities, if sometimes distinct demographics: whereas public schools that serve up to 90% of American children–just short of 51 million (50.8) by federal projections–open for restricted hours if at all, private schools possess the needed funding for on-staff epidemiologists, thermal scanners, and additional teachers–as well as often enjoying more space.
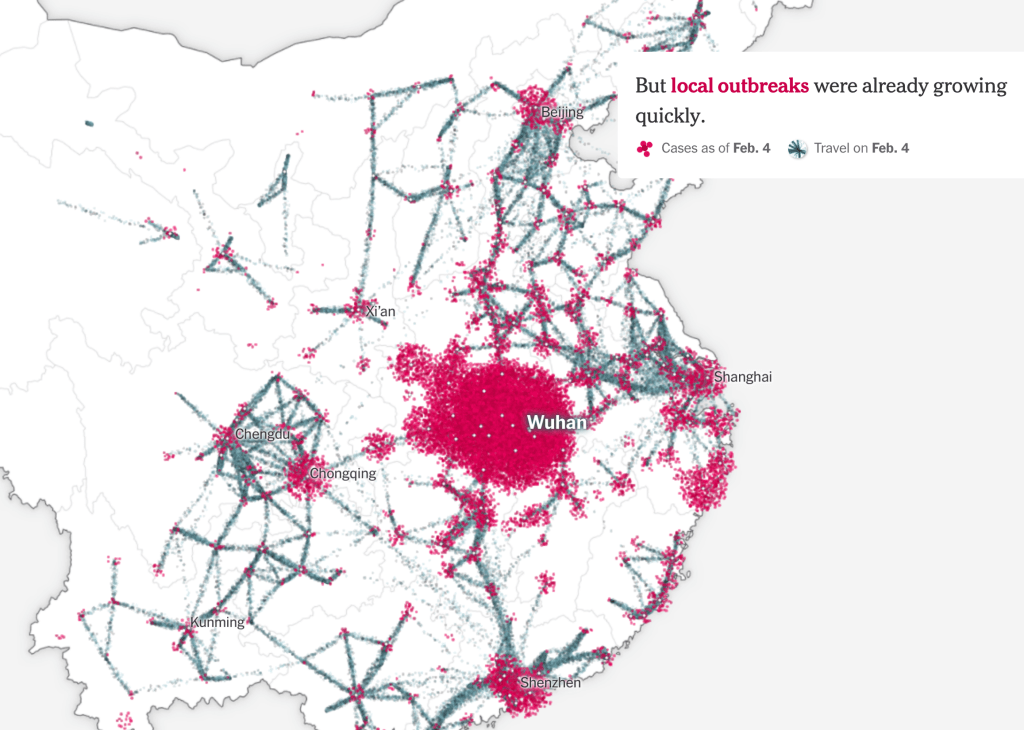
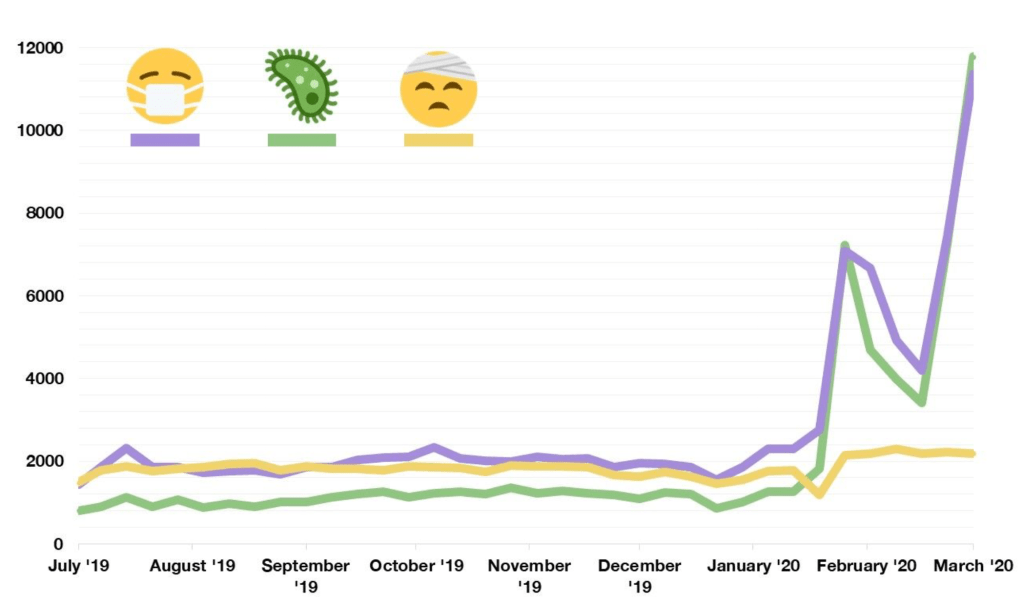
The Emoji Icon Index tells at that on Instagram, the story of a skyrocketing use of the 😷 emoji from early March, as the. Face-with-Medical-Mask rose in use in parallel to the icon of the virus, but a plan for schools, quickly shuttered in China, was not imagined, as wishful thinking prevailed.
While our nation is prepared to react to the novel coronavirus by high-level cabinet meetings to bail out airlines after summoning executives or the bail out of banks, school are evidently far lower down the list. If Donald Trump prioritized cabinet-level meetings on bailing out the airline industries to ensure the Dept. of Treasury provided passenger airlines $25 billion, cargo haulers $4 billion, airports $10 billion and airline contractors $3 billion as industry lobbyists demanded to recognize a 95% reduction of passengers in response to the epidemic, saw meeting with executives to work out that deal worth the time of health officers and coronavirus response team–

–while he saw no similar body of school executives with whom he might meet in one room around a glistening desk with nametags, mugs of coffee and glasses of water. A past President of the P.T.A. of an Alameda CA public elementary school was familiar with reduced funding of California’s public schools since rollbacks on property taxes, smarted at the clear contrast of inability to prioritize public schooling as part of our national infrastructure. Is it not most probable that the very corporate structure of the airline industry provides a more familiar set of faces to interact earning high incomes, unlike the leaders of the dispersed structure of public schools, or community voices, that Trump is so much more apt to dismiss and neglect?
Or is it that the nation is ready to sacrifice the public schools that are less likely to have the funding, save in wealthier districts in Durham, NC or Charlottesville, VA, echoing lines of a deep class divide? Not only were private schools prepared to devote attention and benefited from technological resources to transition to online platforms in the Spring, but are able to use larger buildings and reduced class sizes to benefit the children who attend them, while the aging ventilations systems of older buildings of public schools lie on the other side of a technological divide that plagues the nation.
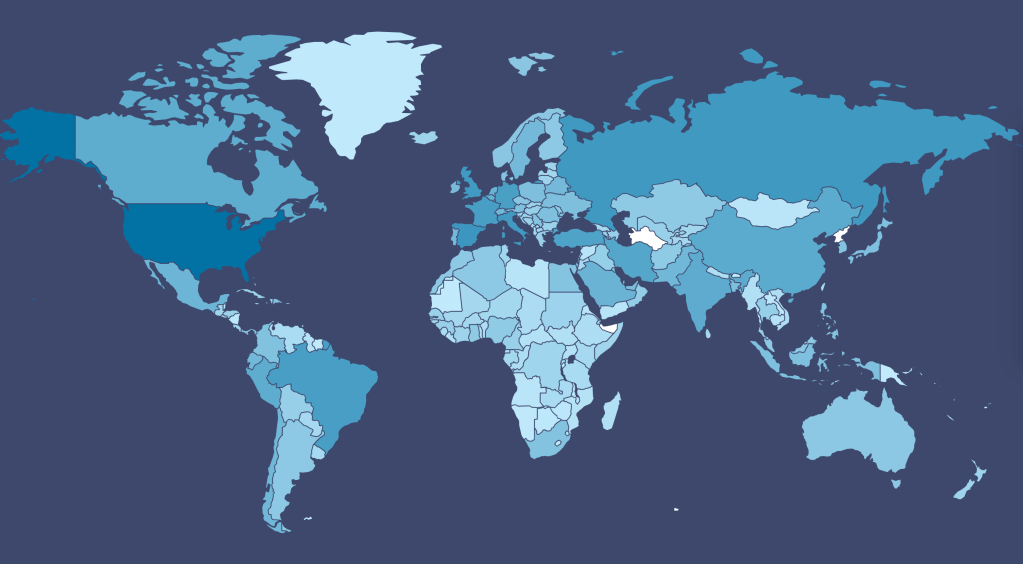
To be sure, there are deep discrepancies–informing the Mapbox Upshot map, of which one might be rightly suspicious given the potentially unsound sampling practices based on the interviews conducted by Dynata, both in the United States and globally, based on 250,000 survey responses between July 2 and July 14; the surveys administered by a firm boasting to provide businesses with a sense of global trends of consumption able to reorient businesses and advertisers to “re-opening,” but while showing vast expanses with relatively lower incidence of a group of five wearing masks–
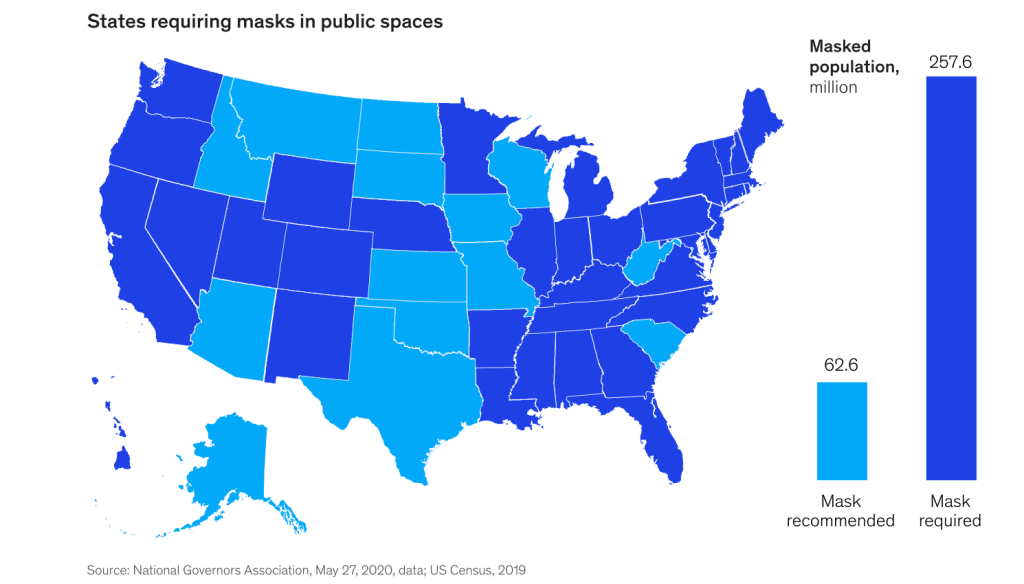
–fails to acknowledge a rift among state governors who recommend masks, rather than require mask-wearing–or the considerable role that mayors have consistently played in advocating mask-wearing, if they often appear over-ruled by governors who have been filling the absence of federal policy: the looses of “recommendations” in Iowa, Wisconsin, Missouri, and Oklahoma, Kansas and the Nebraskas meant that only in some cities, where mayors had advised protective measures, was mask-wearing adopted, creating a terrifying prospect for the pandemic’s future.
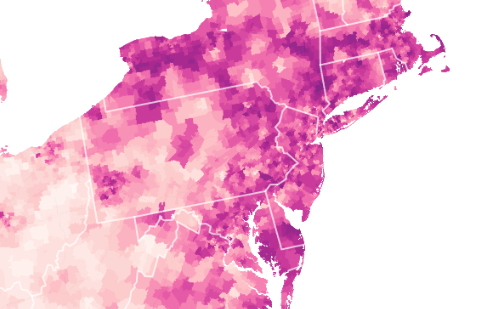
When Fauci addressed the question of health disparities between race, he reminded the nation stoically that “we are not going to solve the issues of health disparities this month or next month . . . but what we can do now, today,” the voice of reason was probably far less reasonable for many, who had already tuned out, before he described the need for social distancing that was, in fact, a privilege for many. The mottled nature of northeastern communities the Dynata found in its interviews suggested an uneven terrain of mask-wearing policies, even in the Tristate Area, dictated by individual choice–and underscoring the lack of regional or federal policies.
The social topography of crowding, of second homes and of gardens or access to parks that was revealed in the Bay Area made us think in practical terms to egregious inequities that were perpetuated by sustained lack of investment to resolve pronounced racial disparities in health came as COVID-19–and the uneven landscape revealed as the coronavirus tore through communities where it was contracted in the United States. The revelation of inequalities was striking, as it suggested how communities experienced it quite differently, and the question of access to education–and access to remote education–cut across social divides in profoundly different ways.
The almost purposeful pronounced lack of master narrative in confronting COVID-19 was long apparent. President Trump, grasping for authority as a true authoritarian playbook, argued the situation demands force, as his removed son-in-law, the dauphin Jared Kushner, spun 60,000 deaths from COVID-19 as a “great success story,” as if to challenge the nation’s personal narratives with a monolithic storyline of a disconnect from communities which were ravaged by hospitalizations. In claiming his father-in-law created a “pathway to safely open up this great country,” Kushner radiated overconfidence as he painted a future as rosy as the marble atrium of Trump Tower, even when the figures didn’t add up. It was akin to Trump’s 1993 proclamation, after huddling with bankruptcy lawyers to obtain new lines of credit, having had “the most successful year I’ve had in business!”–he reprised in a compulsive act of boosterism over the next decade, and continues to rely upon in the pandemic.
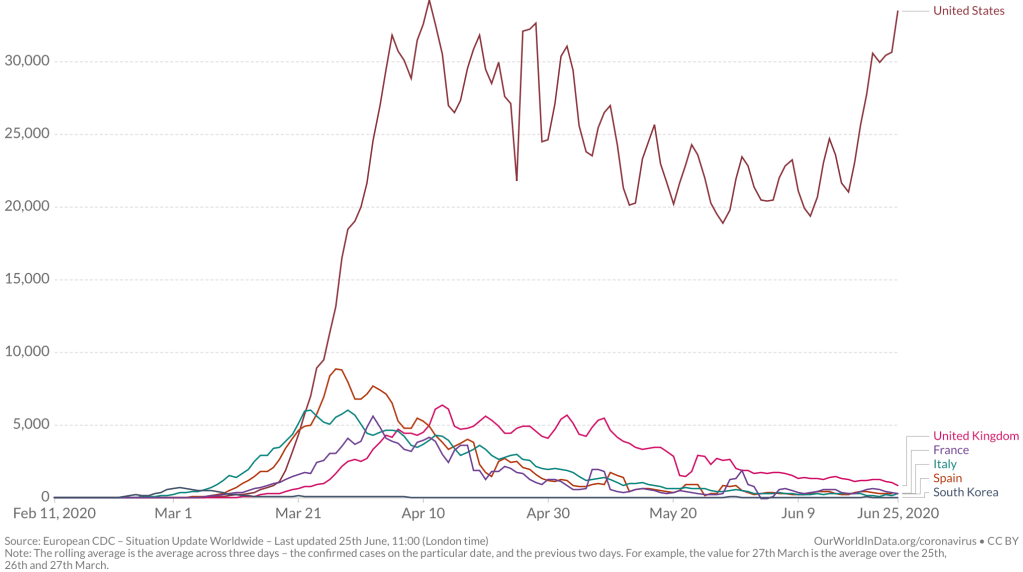
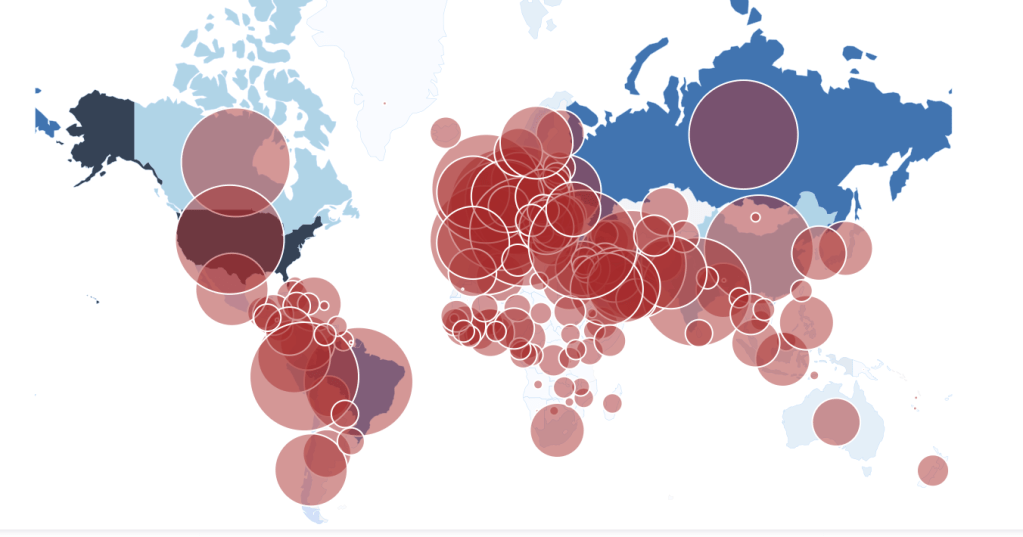
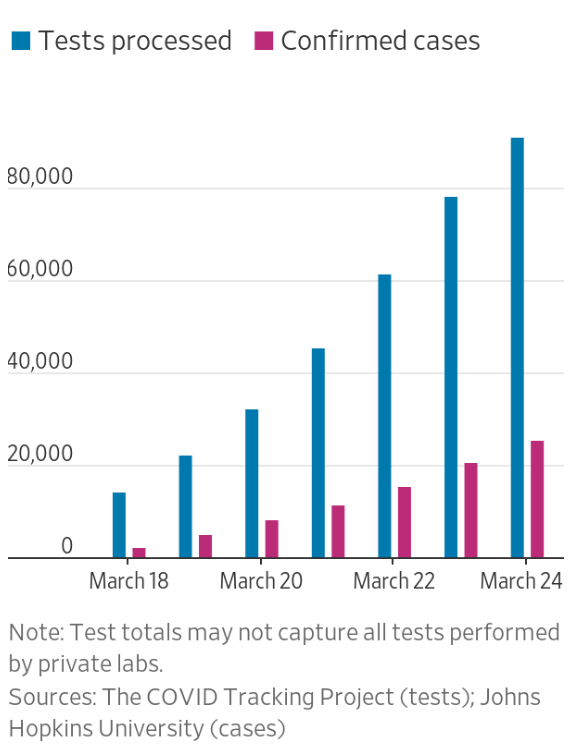
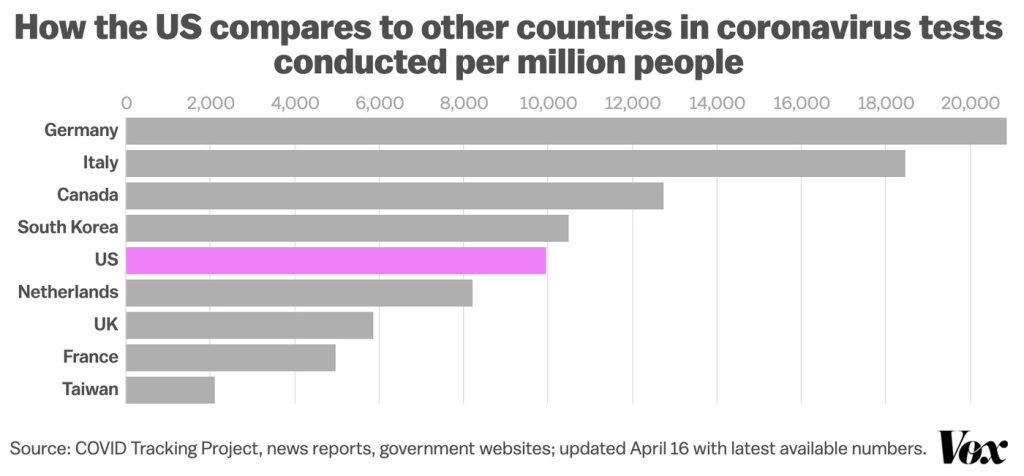
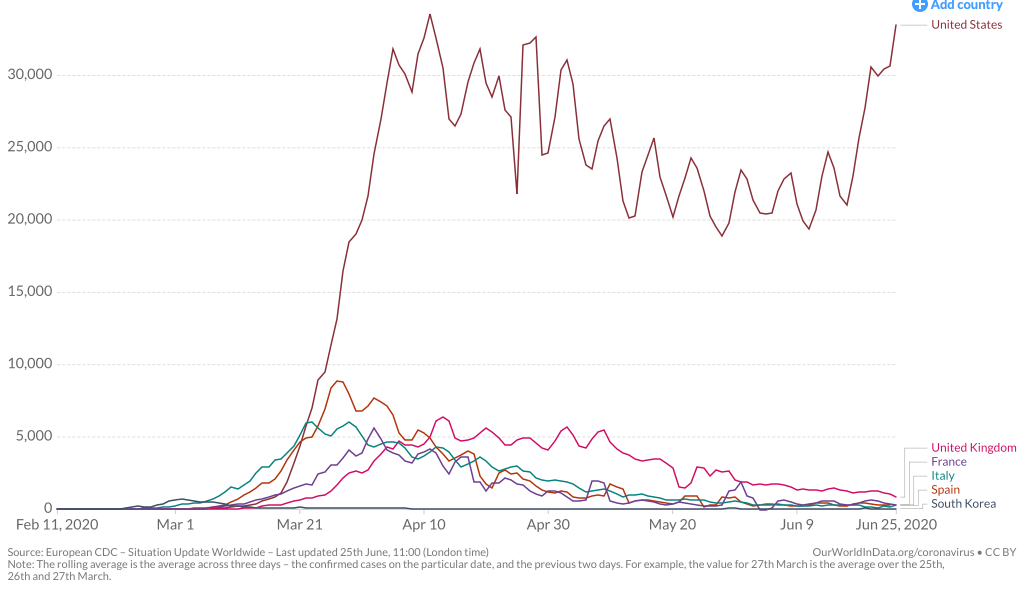
The dauphin Jared had not only used a spilt infinitive, but a split reality, a divergence destined to make the Presidential Election about COVID-19, whose malevolence is hard not to say: as the growth of rates of infection by the novel coronavirus most rapidly grew in the United States, claims Trump was doing “things right” with coronavirus testing plummeting to 30% percent, over twenty-five million unemployed and further furloughs coming, and one million infected by the coronavirus and 60,000 dead in a month, hardly fit narratives that suggest “great success,” even as the rates of infection from the coronavirus may have by mid-March grown greater in the United States than any place in the world, as escalating infection rates would continue to elevate the United States far beyond other nations. The manifestation of symptoms of COVID-19 grew two weeks after contracted, and by late March through late June, they had risen above all other nations.
Yet no clear plan for school closures had emerged on a national level in the United States, and denial at the danger of the infection’s growth dominated. Vice President Pence adopted similar talking points, in a few months, taking it upon himself to bestow premature congratulations that “we slowed the spread, we flattened the curve, we saved lives,” in a mismatch evident to any map in news media, but to the actuality on the ground.
Continue reading